Image-guided therapy
Image-guided surgery uses medical scans, computing and tracking to make treatment more efficient and less invasive and less riskful for the patient. Parts of Image-guided therapy include image- guided radiotherapy and image-guided surgery.
For a general description of imaging techniques, please have a look at the article Brain Tumor Diagnosis.
Image-guided radiotherapy
Image-guided radiotherapy (IGRT) is used to counteract variations in the brain that occur over time.These can include changes in size, location, volume and shape of the tumor. One possibility in IGRT is to get control images (2D X-rays or CT scans) and adjust the therapy plan afterwards. A more modern method integrates the imaging device into the linear accelerator. Then pre-therapy images are compared to images produced during therapy. This allows an immediate correction of the dose and target of radiation dose after automatically analyzing the produced medical images. There are linear accelearators that include CT imaging, as well as some which include MRI imaging. IGRT is useful for the treatment of tumors that are close to sensitive parts of the brain. This advanced therapy can increase the quality of life of tumor patients due to shorter treatment times and higher accuracy in treatments. [6] [7]

Figure 1: MVCT-guided linear accelerator [14]
Tracking systems: There are different approaches to track the patients head and used tools during surgery, which are described in the following. All systems however contain probes on the instruments and the patients and a receiver. The receiver forwards the obtained position information to the tracking system.
- magnetic: mainly used during minimal invasive surgery when endoscopes or needle tips have to be tracked; consists of sensor and field generator; no in-line sight is needed; limited due to the presence of metal in the OR [8]
- ultrasonic: needs sight-lines between probe and receiver;
- optical: needs sight-lines between probe and receiver; retro-reflecting patterns are attached to the probes, which are recognized by multi-camera optical imaging systems.
[3]

Figure 2: schema of magnetic tracking [8]
modern research/ applications
Most research inlcudes a combination of image-guidance and intra-operative images.
Drug delivery though the Blood Brain Barrier (BBB): A lot of research is done lately to improve the drug delivery to the CNS. Many methods focus on breaking/interrupting the BBB. However these techniques affect the whole BBB and therefore increase the risk of unwanted substances reaching the CNS. To lessen these risks, a study on rats from 2005 suggests a MRI-targeted focused ultrasound induced disruption of the BBB, followed by drug delivery to the CNS and MRI imaging to evaluate the amount of the BBBs disruption. First of all, the target of the BBB is set on pre-operative MRI images. The resulting coordiantes are converted to an ultrasound sonication positioning system. This ultrasound system then projects a focused beam to the target in order to harm as little as possible of the BBB. After the ultrasound, intra-operative MRI images are taken in real-time to analyse the disruption of the BBB. [4]
Fluorescence image guided tumor resection: Intra-operative Fluorescence imaging can have a high impact on resecting tumors, espeically high-grade ones. Due to small, diffusive tumor cells at the border of the tumor, these cells can neither be seen on CT/MRI scans, nor through a microscope. Therefore, the tumors have a high chance of recurrence, even after "complete resection". Studies show, that the marker ALA-PpIX is useful to show the diffusive borders of tumors. To examine this behaviour, rabbits with tumors underwent surgery. A few hours before surgery, the marker was injected. Then during surgery the visible part of the tumor was removed with white light resection. Afterwards intra-operative fluorescence image were taken and the remaining visible part, due to fluorescence, was resected as well. To see the marker, the microscope used by the surgeon was adapted for fluorescence imaging. The results of this study suggest that White Light Resection combined with Fluorescence Guided Resection indeed removes more tumor tissue than White Light Resection alone. [5]
MRI-guided laser ablation: Laser ablation is an rising procedure to kill tumor cells with heat. Through image guidance via MRI scans, the tumor can be targeted in real-time and thereby sparing healthy tissue[12]. For more see here.


Intraoperative Imaging
Intraoperative images are used as additional information for the surgeon to detect changes during surgery. Different imaging modalities are in use in today's intraoperative imaging.
Overview over modalities
MRI: Intraoperative MRI images can be produced using different devices, where most of them work in a low-field spectrum. In a special purpose horizontal bore 0.5 T superconducting magnet system, the patient lays inside a double donut. This system gives only little constraints to the access to the patient. Similar impacts hold for general purpose 0.2/0.3 T permanent or electro-magnet systems. In one of this systems, pole-pieces are integrated into the OR table and the field can be raised when needed. In contrast to these systems, conventional 1.5 T systems can be used in the OR as well. These show better quality in the resulting images due to a stronger filed. However, images can only be taken between surgical steps because the patient has to be put inside the magnet. So for the use of MRI, the surgeon has to weight the trade-off between image quality and extra time and effort for producing the images. In general, magentic fields in the OR can introduce a potentially unsafe environment. Further steps indicate the integration of MRI imaging with surgical robotics. [3]
CT: Intraoperative CT scanning takes place with the help of a C-arm. These devices make it possible to take CT images during surgery without moving the patient to another area of the OR room, as for MRI scans. These CT scans can then be compared to pre-operative ones to posibbly adjust the surgical procedure.
Ultrasound: Ultrasound is commonly used for intraoperative imaging because it is cheap and enhances minimal risks. It can detect changes in the patients brain and update pre-operative CT/MRI images. However the ultrasound transducer has to be in direct contact with the brain tissue, which can restrict the work of the surgeon. [3]
Fluoroscopy:A sequence of X-ray scans can be used to see movement of for example the blood vessels inside the brain. By using a mobile system, the scans can be taken without moving the patient during surgery.


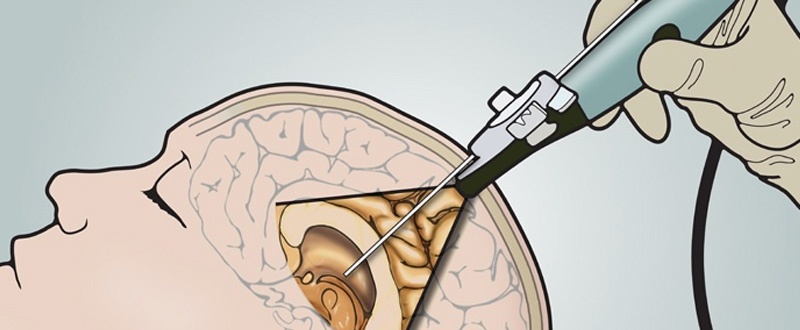
Figure 6: schematic of intraoperative Ultrasound [17]

Research on intraoperative MRI
Brain shift describes the deformation of the brain due to surgical practices. After brain-shift, the preoperative images don't resemble reality anymore. So if the surgeon works with reference to the preoperative scans, e.g. during tumor resection, he could miss tumor tissue and cut out healthy brain tissue. Intraoperative MRI imaging is used to incorporate this shift. In one method, the intraoperative MRI images are combined to a 3D model and registered with the help of bone fiducial markers attached to the head. Afterwards the new images are combined with the preoperative images in a neuronavigation system, which was updated acording to the difference between both images. Results from this trial show that the use of intraoperative MRI images led to a total resection of the tumor in 14/16 tumors. In the two other patients, the tumor grew into sensitive brain tissue, so that it was partly inoperable. So this system shows a reliable navigation with high accuracy, compared to a system without measuring the brain shift through MRI images. [13]
Image Registration/Image Fusion
Overview
Image registration (i.e. geometric alignment) is the process of registering preoperative images and intraoperative images into the same reference frame (i.e. registration of a virtual patient and a real patient). During registration, data sets from different planes, different times (serial registration), different imaging modalities (multi-modal registration), one patient (intra-subject) or multiple patients (inter-subject) are spatially matched. This allows the combination and refinement of anatomical, functional and metabolic imaging. [9] [11]
Rigid image registration uses landmarks. Because many parts of the anatomy are constantly moving, finding fixed landmarks is troublesome. Fiducial markers address this problem: they can be added either on the skin – and may move with the skin – or directly on the bone. The markers can then be found in the preoperative and the intraoperative images and both image types can be combined. Rigid image registration can be applied when the images that are to be matched only differ in rotation and translation. [9]
Usually, registration is complicated by the anatomical changes during the surgery and regular deformations of the anatomy (e.g. because of breathing). Non-rigid registration aims at these deformations by stretching and warping the preoperative image to the intraoperative image. [9] There was a lot of research during the last years in non-rigid registration, but currently they lack the robustness for clinical practice. [10]
Image registration
Image registration means finding the optimal geometric transformation that maximizes the correspondences between two images. Rigid and non-rigid algorithms consist of the following three main components:
- Transformation model: the transformation model defines transformation between the images. In case of a rigid registration, it only performs rotation, translation and scaling (i.e. linear transform). In case of a non-rigid registration, every location pixel/voxel is moved to the transformed location by a displacement vector field (i.e. not a linear transform). Non-rigid registrations are usually smooth and invertible, resulting in non-collapsing structures within the image model. That means that the size and shape changes, but not the topology. In surgery, this is not the case and would need an other approach. For non-rigid registrations, there are parametric and non-parametric models. In parametric models , the displacement vector field for all image points is associated with one discrete 3D grid. Therefore the displacement is a general displacement to a specific location. In non-parametric models, the displacement vector is calculated for each voxel.
- Similarity metric: the similarity metric measures the degree of alignment between images. Intensity-based registration and feature based registration are the two main methods. Intensity-based registration is the main method in rigid registration and compares image intensities to measure alignment. Feature-based registration is better for multi-modal registration and measures the distances between specific features (especially landmarks).
- Optimization method: the optimization method maximizes the similarity metric using numerical methods.
Research on non-rigid registration
Non-rigid registration methods are especially useful to track changes over longer periods of time (e.g. for diagnosing cerebral atrophy) or to correct unwanted motion between two images (e.g. enabling longer acquisition time for intraoperative MRIs, resulting in better reslutions). In one application, in-utero imaging of fetal subjects was performed. To correct the movements of the fetus, non-rigid registration was used (cp. fig. 4).
Non-rigid registration algorithms currently are too slow for a real clinical use. Advances in GPU speed might enable them to be real-time capable, though. Another problem is the validation of non-rigid registration algorithms. Often it is not known, if the patient moved at all, where the patient moved and how much. A standardized validation technique still needs to be developed.

Figure 4: motion correction for in-utero imaging of fetal subjects [11]
Further readings
Here, we listed some papers that might be interesting for further reading/discussion, but which we were not able to review due to time limitations.
Bibliography
[1] https://med.nyu.edu/neurosurgery/physicians/a-z-technologies-guide/image-guided-surgery
[7]Nam P. Nguyen, Mai L. Nguyen, Jacqueline Vock, Claire Lemanski, Christine Kerr, Vincent Vinh-Hung, Alexander Chi, Rihan Khan, William Woods, Gabor Altdorfer, Mark D’Andrea, Ulf Karlsson, Russ Hamilton and Fred Ampil Potential Applications of Imaging and Image-Guided Radiotherapy for Brain Metastases and Glioblastoma to Improve Patient Quality of Life; published in frontiers in oncology (2013); DOI: 10.3389/fonc.2013.00284
[13] Christopher Nimsky, M.D., Oliver Ganslandt, M.D., Peter Hastreiter, Ph.D., and Rudolf Fahlbusch, M.D.; Intraoperative Compensation for Brain Shift; published in Surgical Neurology (2001); DOI: 10.1016/S0090-3019(01)00628-0
[15] https://healthmanagement.org/c/imaging/news/intraoperative-mri-success-at-tubingen-hospital
[17] http://blog.bkultrasound.com/advantages-of-ultrasound-over-mri-or-ct-in-neurosurgery
[18] http://realspinesurgery.com/spine-surgery/#intraoperative-fluoroscopy
2 Kommentare
Unbekannter Benutzer (ga83mor) sagt:
06. Juni 2017Feedback from group 2. Good job guys, well structured and easy to read. I was really pleased to see the #Further readings. The only thing I would say I am not sure that it was worth to write about image registration, because it is really a huge and non trivial topic and a few paragraphs is definitely not enough.
Unbekannter Benutzer (ga67yur) sagt:
07. Juni 2017Thanks for the feedback!