Frameless Navigation
Frameless navigation, sometimes called “neuro-navigation” is the use of real-time intra-operative guidance during operations on the central nervous system. It is called “frameless” because external frames are not needed to guide the surgeon to the target, improving accuracy and safety. You can see our previous discussion of Frameless Navigation on the Technical 1 page.
Despite the rise of frameless navigation, the use of traditional stereotactic frames fixed to the patients’ skull is still widespread in neurosurgery. Particularly in the implantation of deep brain stimulators and electrodes as well as for brain biopsies and cranial radiosurgery. Although there are concerns that the stereotactic frames are uncomfortable for patients, pain experience surveys have been conducted that show stereotactic frames to be well tolerated by patients (Wang, et al., 2014). Nonetheless, the frame has to be applied under local anaesthesia using intravenous sedation.
An interesting consequence of the declining use of stereotactic frames is that trainee surgeons are less exposed to frame application methods which could lead to an increase in complications.

Figure 1: Positioning of the Stereotactic Frame on a Patient (Source: Safaee, et al. (2016))

Figure 2: Comparison of preoperative (A) and intraoperative (B) magnetic resonance imaging to demonstrate shift and decompression encountered during surgery (Source: Orringer, et al., (2012))
Stereotactic Frame Fixture
The fixture of the stereotactic frame to the patient is a relatively straightforward process. The following steps are adapted from Safaee, et al. (2016).
- The frame is positioned on the patients skull using cotton gauzes and spacers to change the height of the frame.
- The pin and screw entry sites are marked on the patient with a marking pen and the frame is removed.
- The patients eyes are covered and a topical anaesthetic (ethyl chloride) is sprayed onto a pin site followed by the injection of a local anaesthetic.
- This is repeated for all of the pin/screw sites needed for the frame.
- The frame is then repositioned and the distance between the skin and bar at each screw/pin is fixed. The pins/screws are inserted on opposite sides and then tightened by hand and then using a torque wrench.
The use of stereotactic frames can lead to a number of complications, including pin site infections and damage to cranial implants, for example the frame has been known to cause deformations in titanium mesh implants (Safaee, et al., 2016).
Frame vs Frameless
There are some proponents of frame-based approaches which claim that although both frame and non-frame based techniques are equally effective for use (here, in intracranial biopsies) the frame-based approaches were shown to require fewer anaesthesia resources and produce shorter OR times (by approximately an hour) and hospital stays for the patient (Smith, et al., 2005). Contrastingly, proponents of frameless approaches make similar claims about their technique – specifically in shorter OR, and anaesthesia times as well as shorter hospital stays (Dorward, et al., 2002). In addition, Dorward, et al. (2002) finds that the complication rate for frameless biopsies is less than for framed biopsies.
Advantages & Disadvantages
There are other advantages to frameless approaches (Lobão, et al., 2009):
- More comfort to the patient due to the lack of stereotactic frame
- Same levels of complications and diagnostic efficiency as framed approaches (see also Dammers, et al. (2008))
- The surgical instruments used in frameless approaches occupy less space than those used with the frame
- The trajectory of the biopsy needle can be changed at any time during the surgery without new calculations being needed
There are of course disadvantages too (Lobão, et al., 2009):
- Precision is closely related to the pre-operative imaging
- Requires accurate registration, depending on the method used for the registration navigational accuracy can be reduced
- Is usually done using general anaesthesia which carries higher risks to the patient than framed methods which use sedation and local anaesthesia.
- The use of general anaesthesia reduces the ability for the doctors to perform a neurological evaluation immediately after the procedure.
- The costs of acquiring a frameless system are high, which can be a barrier to their use, particularly in emerging countries. Note though that the long-term cost (accounting for reduced complications etc.) is lower.

Figure 3: An MRI showing circular fiducial markers on the skull (Source: Cedars-Sinai Medical Center)
Whether the relative advantages and disadvantages of framed and frameless surgeries make one method better than the other is still a topic of debate.
A better conclusion is that framed and frameless methods are complementary systems suitable for use in different situations (Raabe, et al., 2003). The surgeon should decide which is the appropriate method to use. The methods are certainly different in terms of the imaging information required and ergonomics.
Frameless approaches require very high quality images in order to achieve a accuracy comparable to frame-based systems. Using low quality imaging and fiducial markers (e.g. adhesive markers) for patient-intraoperative image registration makes frameless stereotaxic less accurate than framed methods (Raabe, et al., 2003).
Consequently, it is recommended by Raabe (2003) that frameless methods be used for large lesions, i.e. those > 10mm whilst frame based approaches should be used for lesions < 10mm. A similar study in Brazil (Lobão, et al., 2009) came to the same conclusion that framed surgeries were still superior for lesions < 10mm in size. Another study (Bjartmarz & Rehncrona, 2007) also finds that frame-based stereotaxy has higher precision and is therefore better for reaching a small surgical target, however they also suggest that since the frameless technique is more flexible and less dependent on patient form it could be used as an alternative for patients which are excluded from frame-based surgeries for technical reasons.
Accuracy
The important factor for both methods is achieving the highest accuracy possible as the amount of tumour that is resected is directly related to improved patient outcome, see for example Smith et al. (2008) for a study in this regard on low-grade gliomas.
A common way to measure the accuracy of the different framed and frameless systems is in an operation for the implantation of deep brain stimulation (DBS) electrodes for treating patients will movement disorders. Commonly, the electrodes are inserted using either a framed or frameless approach and then an X-ray is used to verify the final electrode positions and deviations from the planned target are measure from this image.
A 2007 study (Bjartmarz & Rehncrona) of electrode implantation using a common stereotactic frame and frameless system (Leksell and Nexframe respectively) found that the frameless technique was less accurate, having a vector accuracy of 2.5 +/- 1.4mm vs 1.2 +/- 0.6mm for the framed based technique. The same study found that the dispersion was larger when a frameless technique was used.

Figure 4: Comparison of accuracy in different patient axis of framed and frameless DBS electrode placement (Source: Bjartmarz & Rehncrona (2007)).
Bjartmarz & Rehncrona suggest a number of reasons for this outcome have been suggested. First, in the frame-based approach the brain is registered from the beginning in relation to a skull-fixed frame using a computer planning system with six different MRI indicators; whereas in the frameless system has fewer markers for registration. Additionally, the position of the markers has to be verified by hand by the surgeon. It is though that the increased number of interfaces and information transfers may make the frameless approach more susceptible to error.
Second, in the frame-based approach the surgical target is always located in the center of a sphere and the trajectory is a radius with its movement axis in that location. Contrastingly, the frameless approach has its movement axis close to and above the skull bone to facilitate better movement in the surgical target area. This means that if there is any instability in the frameless system then the small angular variations this would cause can have a large effect on the final location of the electrode.
Interestingly, despite the differences in electrode placement the clinical outcome was the same with both techniques – that is the tremor reduction was similar for both framed and frameless techniques. Although this means that either approach can be used for this treatment Bjartmarz & Rehncrona note that this does not necessarily hold true for other surgical procedures where there are smaller targets, requiring higher accuracy to achieve a clinical effect.
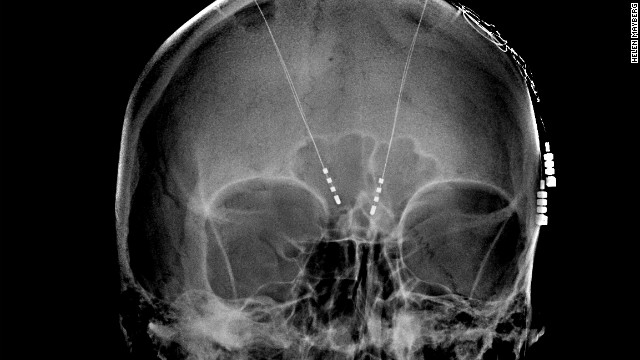
Figure 5: CT showing electrodes planted inside the brain to treat depression (Souce: CNN).
Despite the findings of Bjartmarz & Rehncrona (2007) a number of later studies have found different results. For example a larger study by Bot, et al. (2015) found equal accuracy (not statistically significant) of both framed and frameless approaches using the same equipment as in the Bjartmarz & Rehncrona (2007) study. Although the overall 3D accuracy (euclidean accuracy) of both systems was found to be the same there is still different variation in different axis.
Bot, et al. (2015) also noted a number of other advantages of the frameless approach which have not been discussed so far. The first point is that the use of the standard stereotactic frame requires imaging to be performed on the day of the surgery whereas the bone fiducials used in the frameless approach can be placed and the imaging performed prior to the day of the surgery. This allows planning before the surgery as discussed, but also reduces the possibility of the patient become exhausted during the already lengthy DBS surgery – thereby increasing their ability to cooperate with the surgeon. The splitting of operation and imaging time also means the patient spends less time off their medication (required for the surgery).
Another point mentioned is that the particular frameless system used (Nexframe) consists of disposable components. For stereotactic frames which are not disposable the frame has to be periodically recalibrated to detect and correct systematic errors which accumulate with every operation. Whereas the frameless solution is calibrated when it is unpacked and since it is disposed after the surgery there is no chance of systematic errors from repeat usage. Stereotactic frames also require sterilization after the operation, thus the number of electrode implantations a hospital can perform is limited to the number of stereotactic frames they own. By contrast, with disposable frames more procedures can be completed per day.

Figure 6: The Nexframe platform with attached microdrive (Source: Khan & Henderson (2013)).
Other Factors Affecting Accuracy
Registration Method
Frameless stereotaxy requires a registration to be made between the pre-operative and interoperative images. One of the main ways this is done is using fiducial markers and a point-pair registration but anatomical landmarks can also be used as can surface matching. Each of these registration approaches has a different accuracy. This accuracy is given as the target registration error or TRE which is the Euclidean distance between the image space coordinates and world space coordinates of a target marker. The target marker is separate from the registration markers and is used to simulate a surgical target.
A study by Woerdeman, et al., (2007) found that regardless of the target location or imaging modality adhesive markers were the most accurate way of performing a registration with mean accuracy of 2.49mm compared to 5.03mm for surface matching and 4.97mm for the use of anatomical landmarks.
Of course, fiducial markers can only be used for planned registration where the patient has the markers placed before being sent for imaging. If images from earlier studies are used then anatomical landmarks and surface mapping can be used.
Registration Sequence
It has been found that when scalp fiducial markers are used for registration there is no impact on accuracy of the order in which the markers are registered (Smith, et al., 2014).
Marker Arrangement
Fiducial arrangements distributed optimally across the skull, however, allowed for significantly improved accuracy.
When using fiducial markers a number of errors can occur (Smith, et al., 2014):
- Fiducial localization error – the difference between where a fiducial is in the image space and where it is in the patient space, e.g. due to movement of the markers between imaging and surgery.
- Fiducial registration error – the difference in position after the marker has been registered (reflects the variability of the registration system).
- Target registration error (TRE) - the error in measuring a target once a system is registered.
Of these errors, the most important is the TRE as it determines how confident the surgeon can be when relying on the image guidance.
Smith, et al., (2014) conducted a study whereby they arranged the fiducial markers on a phantom in a number of different arrangements in order to see if the marker placement had an impact on accuracy as measured by the TRE. The arrangements they tested (in addition to 3 random arrangements) were:
- Axial – a band around the head in a coronal plane
- Bifrontal – markers only across the frontal region
- Coronal–sagittal - one line of markers in a single sagittal plane and another in a single coronal plane
- Parasagittal - bilateral lines in parallel sagittal planes
- Two-axis - two different bands around the head in parallel axial planes
- Wide-whole – markers spread across the whole skull
They found that the most accurate arrangement was two axis with a TRE of 1.35 mm +/- 0.065mm. The wide-whole arrangement also performed well (1.43mm +/- 0.061mm) and both performed better than the other arrangements. It is suggested that this is due to the wide distribution of markers in these arrangements which have very little redundancy. This is an important result as it means fiducial marker placement needs to be performed more precisely and taken into consideration when performing or planning a surgery. Particularly since different arrangements may be better in different treatments (West, et al., 2001).
West, et al., (2001) found that for cranial neurosurgery the best approach is to use widely spread fiducial markers as well as placing the markers near to the target. For a different surgery, pedicle screw placement it was found that the best approach was to avoid using collinear markers.
Future Developments
Stereotactic Mass Spectrometry (Agar, et al., 2013)
Across a range of brain tumor types and grades, postoperative residual tumor has a great impact on prognosis. The principal challenge and objective of neurosurgical intervention is therefore to maximize tumor resection while minimizing the potential for neurological deficit by preserving critical tissue.
Using a frameless stereotactic sampling approach and by integrating a 3-dimensional navigation system with an ultrasonic surgical probe, we obtained image-registered surgical specimens. The samples were analyzed with ambient de-sorption/ionization mass spectrometry and validated against standard histopathology. This new approach will enable neurosurgeons to detect tumor infiltration of the normal brain intraoperatively with mass spectrometry and to obtain spatially resolved molecular tissue characterization without any exogenous agent and with high sensitivity and specificity.
The mass spectrometry measurements reflect a complex molecular structure and are integrated with frameless stereotaxy and imaging, providing 3-dimensional molecular imaging without systemic injection of any agents, which can be implemented for surgical margins delineation of any organ and with a rapidity that allows real-time analysis.

Figure 7: Components of a Stereotactic Mass Spectrometry System (Source: Agar, et al., (2013))
Pantograph Stereotactic Localization and Guidance System (Abrishamkar, et al., 2011)
Both frame-based and frameless guidance systems have different advantages and disadvantages. In order to get the “best of both worlds” some hybrid systems have been designed. These aim to combined the instrument carrying and stability of frame based methods with the flexibility of frameless methods such as the ability to change the trajectory or surgical target during the operation.
One such system is the “Pantograph Stereotactic Localization and Guidance System” (Abrishamkar, et al., 2011) which uses a pantograph to map movements made on the guidance display to movements made on the patient. A pantograph is a mechanical linkage connected so that the movement of one ‘pen’ produces an identical movement in another. Here one ‘pen’ is used to trace the pre-operative images on an LCD screen whilst the corresponding motion is made on the patient.
The pantograph system is less bulky than a full stereotactic frame whilst still being able to support all the devices a surgeon might need during the operation. This gives the surgeon more freedom to move about in the operating area whilst being able to navigate flexibly. A pantograph system is also easier to use than complex frameless navigation software and also less expensive so can be used in developing countries.

Figure 8: Pantograph Stereotactic Localization and Guidance System (Source: Abrishamkar, et al., (2011))

Figure 9: Propsed set up of frameless radiosurgery system. The bar behind the patient (184) is an additional infrared tracking system for monitoring breathing or other motion made by the patient. This complements the X-ray tracking of the target (106) (Source: Radler (2004))
Frameless Radiosurgery (Radler, 2004)
It is important that radiotherapy is performed in an accurate manner so that healthy tissue around the surgical target is not harmed. This was, and usually still is, achieved using a frame-based method where the frame is used to targeting and immobilization of the patient. Preventing the patient from moving during the surgery is an important part of ensuring the targeting remains accurate.
Frame-based methods work well for the brain, though do have other issues, but most parts of the body do not have such a large bone structure as the skull, so it is difficult to attach a frame for treatment of cancers in other parts of the body (Radler, 1993).
Another issue with the frame-based approach however is that it cannot be used for fractionated treatment plans. In such a treatment plan, small doses of radiation are repeatedly given to the patient over time, which may be weeks or months, often with a rest period in between doses to allow healthy tissue to heal. Fractionated radiotherapy is desirable both because it allows healthy tissue to heal by also because it allows a larger overall dose to be given to the patient.
Frame-based approaches cannot be used here because it would not be possible to leave the frame attached to the patient between doses, nor can it be reattached later since it could not be positioned exactly in the same location for the next dose.

Figure 10: Accuray CyberKnify Frameless Radiosurgery System with ceiling mounted tracking sources (Source: Accuray).
This can be avoided using frameless radiosurgery which does allow for fractionated treatment plans by incorporating a system for the accurate targeting of the radiotherapy beam. Usually, a preoperative image of the surgical target and surroundings is taken and the target marked. Then intraoperatively two further images are taken using X-ray imaging and formed into a stereo image. This stereo image is then registered to the preoperative image to allow the target to be located accurately. Finally, a robot is used to positioned the therapy beam using the registered intra- and pre-operative images. This results in the beam causing less unnecessary damage to tissue in the surrounding region.
Other advantages of the frameless approach include improved comfort for the patient as well as more efficient use of personnel and equipment since most of the work is now handled by a robot (Breneman, et al., 2009).
There are some drawbacks to this frameless approach, the main one being that the robot required to support the therapy beam and imaging systems is very large, this severely reduces the working space in the OR. Additionally, the cost of having two imaging systems makes the treatment system expensive. Other problems arise when frameless approaches are used on soft-tissue which do not necessarily occur for neurosurgery. One problem here is that to register the pre- and intra-operative images implanted fiducial markers are required as soft tissue is not viewable on the X-ray. The other is that motion, e.g., due to breathing, may reduce the accuracy of the surgical target identification by reducing the quality of the tracking images.
It has been found that the clinical outcome, usually measured as local control after surgery, of frameless radiosurgery systems is high, 89.9% (Bilger, et al., 2017) and comparable to the outcomes after frame-based radiosurgeries (Breneman, et al., 2009). Frameless systems are also capable of achieving the same level of precision in targeting as in frame-based approaches (Murphy & Cox, 1996).
Skull Mounted Trackers (Fanous, et al., 2017)
The first development from frame-based navigation systems was the use of frameless systems based on pre-applied fiducial markers. The problem with marker based registration is that they require additional pre-operative MR images to be taken on the day of the surgery which increases the cost of the surgery. When fiducial markers are used they also require the patients head to be fixed. This re-introduces some of the problems with framed surgeries – namely, it increases the risk of potential skull fractures and limits the surgeons’ flexibility.
To avoid some of these issues facial masks were developed. These do not require pre-operative imaging or fixing of the patient’s head. With a mask based system, a mask with a number of registration points on the face and forehead is applied to the patient. Registration is then performed to the surface of the mask. The disadvantage of the mask-based approach is that the mask prevents a wide sterile field/operating area which is required for certain operations such as the placement of shunts. The mask may also pose an obstacle in surgeries involving the face and forehead.
Skull-mounted tracker kits eliminate the disadvantages of both masks and fiducial markers. In this system, the stereotaxy is initially performed with a facial mask. Then a ‘skull post’ is attached to the patient’s skull and the registration to the mask transferred to the skull mounted tracker. At this point the mask can be removed. By allowing the mask to be removed a large sterile field is available which makes this method useable where the mask would be unsuitable. Skull-mounted trackers allow for the free re-positioning of the head throughout the surgery. In addition to solving the problems of the marker and mask approaches you also get all the benefits of frameless navigation – skull mounted trackers are less time consuming to set up than frames and avoids the complications associated with rigid head fixation.
The typical accuracy of skull based trackers is a tip deviation from superficial and bony landmarks of <2 mm.
Of course, no method is without it’s disadvantages. The main limitation of skull mounted systems is that they can only be used for lesions situated toward the front of the head and base of the skull. This is because since all of the registration points are here which means the precision is reduced at the rear of the skull. Additionally, skull-mounted navigation requires optical tracking. This in turn introduces a requirement for a direct line-of site between the camera and the system which could limit the flexibility of the surgeon as they can’t obstruct the camera.
Electromagnetic Navigation
The problem of optical tracking can be solved through electromagnetic navigation since no direct line of sight is required. Although it has been suggested that iron containing surgical instruments may destroy the magnetic field and create inaccuracy. Additionally, the electromagnetic field produced by these tracking systems is small, so the corresponding surgical field must also be small. This limits the use of such tracking in some surgeries, like shunt placement. Further, as cortical stimulation can interfere with the electromagnetic field it is not possible to stimulate the brain and perform navigation at the same time (Morsy & Ng, 2015).

Figure 11: A skull-mounted tracking system for frameless neurosurgery (Source: Fanous, et al., 2017).
Electromagnetic (EM) navigation has been successfully used in awake craniotomies. An awake craniotomy is identical to conventional craniotomy in practically every way, except the patient is awake and able to respond to the surgeon during the procedure. This is the preferred neurosurgical technique for operations to remove lesions close to functionally important parts of the brain as it allows the patients neurological function to the tested continuously throughout the operation which reduces the risk of damage to important tissue (University Hospital Southampton, 2014).
Morsy & Ng (2015) found that EM navigation provided the same accuracy as optical navigation with the benefit that the patient did not need to be fixed nor did the surgical tools interfere with the tracking. Considering that the patient is awake for awake craniotomies it is also important that they are as comfortable as possible which is aided by not having their head fixed – the small size of the EM sensor allows free head movement. This is not only advantageous to the patient but also to the surgeon as it means that the head can be rapidly repositioned to allow for airway access and protection if an emergency arises during the procedure.
EM navigation also compared favourable to infrared navigation systems as the sensors (copper coils) can be very small, on the order of several millimetres. In contrast, an infrared (IR) system required a number of emitters and reflectors separated by several centimetres to achieve the same sort of accuracy, thus making IR systems impractical if the patient is not rigidly fixed (Morsy & Ng, 2015).

Figure 12: Intraoperative microscope with attached frameless navigation system (blue arrow) (Source: White, et al., 2017)
Frameless Navigation and Microscopy (White, et al., 2017)
A common problem is neurosurgery is the difficulty of accessing deep targets. This can be done using stereotactic needle biopsies but they often provide a poor tissue sample of have a sampling bias which can lead to a misdiagnosis, especially if the targeted lesion is small. Instead frameless navigation is usually used for targeting together with a surgical microscope. The use of the microscope allows the surgeon to visualize and manipulate fine structures more accurately. This can lead to better samples or more thorough tumour resection.
Currently however, the microscope and frameless navigation system are used in a “serial fashion”. That is to say that the surgeon has to switch between looking at the navigation system (usually on a monitor) and adjusting/looking through the microscope. Continuous visualization with the microscope would increase patient safety by preventing the surgeon from having to look up from the microscope and potentially losing their trajectory.
White, et al., (2017) affixed a commonly used neuronavigational system to the microscope. The navigational system is used to register the microscope to the patient using fiducial markers placed on the patient. As the surgical tool is advanced deeper into the brain the surgeon alters the focus of the microscope thus moving the affixed tracker, allowing the position of the tool to be updated in the frameless navigation interface which is also visible to the surgeon.
This method could see further improvements in the future, currently the surgeon still has to maintain the microscope focus, it would be far better for the microscope to track the tool and focus automatically. Additionally, more visualisation techniques could be built into the microscope. It is thought that in the future, microscopes will also display MR images or CT scans simultaneously and combine the information intraoperatively. This real-time access to imaging data will help the surgeon make decisions during the operation (Uluç, et al., 2009).
Surgical Simulators
A surgery simulator is computer technology developed to simulate surgical procedures. This simulators can be used for the purpose of training medical professionals, without the need of a patient, cadaver or animal. They are best suited for two types of skills needed for surgery, eye–hand coordination and the ability to perform three dimensional actions using a two-dimensional screen as a guide. Eye–hand coordination is improved because the simulation can give both visual feedback, by way of a screen, as well as tactile feedback that simulates the manipulation of organs and tissue. Surgical simulators provide a no-risk environment where skills can be gained through harmless repetition.
“Simulators provide harmless and repeatable practice, multiple and varied scenarios, immediate feedback, uniform standards, objective measures, and trend analysis… For neurosurgery, sophisticated simulators would be a great advance in residency training. Although they are very costly, they could be provided in specially designed training centers. Simulators would be highly useful in the certification and maintenance of certification processes as well as in continuing medical education, refreshment of skills, and even surgical rehearsal.”
(Quest, DO. The 2007 AANS presidential address)
What parts does a simulator usually include?
Although simulation environments vary widely in their procedural applications and implementation details, each can be understood in the context of 3 primary components:
graphics/volume rendering,
tissue deformation/model behavior,
and haptic (force) feedback.
Below we discuss all these components one by one as mentioned in (Malone et.al),
- Volume rendering/ graphics :
Computerized 3D volumetric anatomical models are constructed from medical imaging data. The medical imaging techniques that are used can be computed tomography [CT], magnetic resonance imaging [MRI]. The models are constructed through a combination of image processing and geometric modeling. Volume rendering is used to then display these models in the simulation. Below are some of the rendering techniques used,
Direct rendering approaches: These approaches describe an anatomic structure as a volumetric model. This volumetric model is described as cubic elements known as voxels and use image density values to delineate adjacent tissues. Direct rendering produces a true volumetric reflection of original image. This true volumetric reflection comes at a high processing cost, creating a computational burden that may limit the interactive fluidity of simulators.
Indirect rendering, or surface rendering: These techniques generates models that describe only the surface of anatomical structures.These techniques neglect the internal volumetric data. With this the indirect rendering dramatically reduces computational burden and improves the processing speed of medical simulators. Once a structure has been properly segmented from adjacent tissue, it can be assigned appropriate visual and bio-mechanical properties.
Volume rendering: Volume rendering is a labour intensive tasks when used for the purpose of simulation, in particular, in patient-specific models. In addition to that, the real-time integrated processing of tissue behavior and tactile feedback results in a significant computational burden thus remaining an obstacle in the evolution of surgical simulation.
2. Tissue deformation/model behavior :
To facilitate simulation, volume-rendered models must be capable of responding to user manipulation with virtual tissue deformation. Few techniques of handling model behavior are discussed in the section below,
The mass-spring method is a common approach to tissue deformation in real-time simulators. A major limitation of this method, outlined by Spicer.et.al, is its inability to accurately depict a surgical cut.
The finite-element method (FEM) is an approach to tissue deformation that more aptly accounts for tissue bio-mechanics. FEM represents a structure as a lattice of connected 3D volumetric elements, like cubes or tetrahedra. It then uses a variety of mathematical approximation techniques to solve constituent equations that describe the way that a material being modeled responds to applied forces. FEM can produce models with greater bio-mechanical accuracy than those using mass-spring techniques. Thus, FEM enhances the fidelity of tissue deformation, but does so at a high computational cost that may hinder the fluidity of interactive simulators.
3. Haptic feedback:
Haptics, in the context of surgical simulation, broadly refers to the feedback of sensory information. Sensory information includes tactile, kinesthetic, vestibular, and proprioceptive modalities. Haptic feedback is transmitted to the user via a physical interface that interacts with the computer-based graphic model. This is the integration of what is seen with a realistic sensation of what might be felt. i.e mapping what is seen to how it is felt. To produce realistic haptic feedback, simulation environments must be supplemented with external haptic interfaces. These interfaces should be capable of producing accurate tactile sensations.
Minimally invasive neurosurgery have very limited haptic parameters. This makes it most favorable subject for simulation. An endoscopic surgical field can be recreated by a haptic interface that resembles surgery site. Also, by limiting the degrees of freedom of the instruments, they can move above the port. Endoscopic simulator interfaces provide high haptic fidelity without creating a compelling computational burden.
Model building:
Finding and developing suitable models for the purpose of training a neurosurgeon is always a challenge. There is the need for accuracy and realism, and these have to be balanced against cost, rules, and regulations. Model building can be divided into two parts, Algorithmic and Non-Algorithmic. We will delve into the non algorithmic aspects in the section below as discussed in (Waran et.al).
Non algorithmic:
With the 3D printing in the mainstream, it has become possible to create/ print models using the actual patient data. Also using this patient data to aid in the planning of complex surgical procedures as well as to explain such procedures to patients and their relatives. Latest generation of 3D printers allow models to be created out of materials of varying consistency and density thus adding reality to the models created. A brief description of one such study is mentioned below,
A case study from Waren et.al:
The CT data obtained in a patient with a cortically located brain tumor were selected, and the various tissue components (skin, bone, and dura mater as well as the tumor surrounded by normal brain) were segmented.
The 3D printer was able to create various tissue types of varying consistency and density to mimic skin, bone, dura, and tumor (Fig. 13: composite cross-section). In the programming of the machine’s print characteristics to mimic actual tissue handling, a number of features were considered. The “skin” needed to be pliable enough to be cut by a knife and to hold a suture. An interface layer was created to allow the flap to be raised from the underlying “bone” as in a real patient. The “bone” layer was made solid to provide the feel of using conventional perforators and bone cutters.
An interface was also created between the “bone” and “dura,” thus allowing the cranial perforator to stop automatically when the dural layer was encountered.
The “dural” layer was designed to be lifted off the underlying “tumor.” The space occupied by the “tumor” was printed based on the actual patient’s imaging data. This “tumor” was differentiated from the surrounding “brain” by creating a variation in consistency, the “tumor” being softer than the brain. The “tumor” was colored orange, whereas the “brain” was light yellow.

Figure 13 : Cross-sectional view of model with tumor, and drawing delineating parts of the model. Source : Waran et.al



EDEN 2020
EDEN2020 is a research project centered around developing tools for diagnosis and minimally invasive treatment for neurosurgery applications. The project will focus on 5 technologies:
- Pre-operative MRI and diffusion-MRI imaging
- Intraoperative ultrasound
- Robotic assisted catheter steering
- Brain diffusion modelling
- A robotics assisted neurosurgical product called the “Neuromate”

Figure 17: The EDEN2020 Logo (Source: EDEN2020)

Figure 18: Animation showing CED operation on a dog (Source: Virgina Tech College of Veterinary Medicine).
The main output of the project this a set of steerable catheters that can be used by robots and held in place for long periods of time. A key part of this is that the system can monitor deformations in brain anatomy throughout a neurosurgery and respond appropriately. The purpose of these catheters is for drug delivery to the brain. Consequently, another part of the project is the modelling and prediction of drug diffusion within the brain. This method of drug delivery is known as convection enhanced delivery or CED.
In a typical CED procedure a minimally invasive trajectory to the brain is planned and small diameter catheters are placed directly into the brain tumour. Drugs are then delivered through the catheter over the course of several hours. This approach bypasses the blood0breain barrier and so allows drugs that would not normally cross the blood brain barrier to reach high concentrations within the brain tumour.
As part of EDEN2020 convection enhanced drug delivery will be trailed on sheep through both ex vivo and in vivo studies.
Formally the objectives of the EDEN2020 project are as follows (adapted from EDEN2020 (2017)):
- To engineer a family of steerable catheters for chronic neuro-oncological disease management that can be robotically deployed and kept in situ for extended periods.
Brain disease is a growing problem, particularly due to the aging population. The tools we use for neurosurgeries today are inserted via rigid cannulas which cannot make use of pre-planned and optimized trajectories. The use of pre-planned trajectories is allows the damage to healthy tissue to be limited and to make sure the drug diffuses to the tumour tissue efficiently. The EDEN2020 project will use robotic guided catheters to allow for the use of pre-planned trajectories for better drug delivery in neurosurgery.
2. To control robotic, steerable catheters with enhanced autonomy, surgeon cooperation, targeting proficiency and fault tolerance.
One of the things currently preventing the widespread use of surgical robotics is the difficulty in balancing the autonomy of the robot and the involvement of the surgeon.
Currently, the surgeon needs to be heavily involved in guiding the robot since they lack control strategies that can handle the tissue deformations that occur normally during the course of a surgery. EDEN2020 will develop new cooperative control systems for robotic catheter insertion which use intraoperative sensors to handle tissue deformation, thereby reducing patient risk and improving accuracy.
3. To sense and perceive intraoperative, continuously deforming, brain anatomy at unmatched accuracy, precision and update rates.
It is possible for tissue deformation to be monitored intra-operatively through ultrasound imaging. However, this currently suffers from poor image resolution and other imaging artefacts. The EDEN2020 project aims to develop new parallel processing schemes for capturing and processing ultrasound images and registering them to MRI images for use intraoperatively for guidance.
4. To model, understand and predict drug diffusion properties within brain tissue with unprecedented resolution and comprehensiveness of factors.
The flow of fluid within the brain is anisotropic because of differences in intracranial pressures and inhomogeneity in the distribution of extra-cellular water. These factors are not currently taken into account when modelling drug delivery to the brain. As part of the EDEN2020 project new models will be developed which consider these factors in the hope of improving predictive accuracy.
5. To study in vivo diagnostic sensing in flexible access surgery.
There are new sensors that may be able to enhance neurosurgical procedures by providing the surgeon with more information in real time, for example: tumour boundaries, pathology and anatomical landmarks. The EDEN2020 project will investigate how diagnostic sensors embedded within flexible catheters could improve neurosurgical procedures.
6. To build a unique database of paired clinical datasets (human and ovine) that includes registered information regarding anatomy, white matter tracts, histology and microstructure.
At the moment, there are no publicly available databases that can be used to model drug diffusion in the brain. As part of EDEN2020, such a database will be developed.
7. To create a pre-commercial technology platform for neurosurgical catheter insertion that exploits the technological and clinical outputs of all other objectives.
EDEN2020 will develop the capabilities of the existing neurosurgery assistance robot, the ‘Neuromate’.
Current Research
Robotically Steered Needle Trajectory Planning (Liu, et al., 2016)
Robotically steered needles provide minimally invasive access to surgical targets located deep in the brain. It is hoped that they will improve the efficacy of a number of interventions, including tumour management, whilst reducing patient trauma. Ultrasound will be used to track tissue and needle deformation in real time, intraoperatively so that the optimal insertion trajectory can be continuously updated.
This navigation process is accelerated using GPGPU programming which greatly reduces the latency in the navigation and makes the surgery safer and increases the accuracy.
On the GPU the US images are segmented to separate the needle, target, obstacles and safe tissue. The needle and surgical target are then estimated and the path planner estimates the optimal path (by exhaustive search due to its ability to handle complex anatomy and guarantee path quality), avoiding obstacles to the target and updates the surgical plan as appropriate.
The presence of speckle noise in US images makes the segmentation challenging and so convolutional neural networks are used to perform the segmentation – also accelerated by using GPUs.
Laser Doppler Based Sensing for Blood Vessel Detection with a Steerable Needle (Virdyawan, et al., 2016)
A common complication during neurosurgery is haemorrhaging (heavy bleeding) caused by damage to a blood vessel by the surgical needle. This occurs because not all blood vessels are detected during the preoperative CT or MR scan. Real-time imaging intraoperatively, like ultrasound cannot easily penetrate the skull so it is not possible to detect blood vessels intraoperatively in this way. Instead it is thought that these vessels could be detected by adding a forward-looking sensor (such as a Laser Doppler Blood Flow sensor) to the surgical needle used in the operation. This is being further investigated as part of EDEN2020.
Neuromate® Stereotactic Robot
The Neuromate robot is a 6 joint robotic arm which can be positioned in space with high accuracy (0.7mm) and can stabilise payloads of up to 7kg. The “Neuromate” works an assistant robot. Rather than performing the operation itself, this robot holds and stabilizes tools controlled by the surgeon. This improves surgical safety and accuracy. In particular it has been used to deliver small-diameter catheters to the brainstem together with real-time MRI tracking of drug diffusion distribution (Barua, et al., 2013).
A potentiometer in each joint of the robot measures the current joint angle allowing the robot to be positioned by a computer which also registers the robots position with the patient. The Neuromate is used in stereotactic neurosurgery in conjunction with the traditional stereotactic frames.
However a ultrasound registration system can also be used which eliminates the need for the traditional stereotactic frames. So far this has been shown to be comparable in accuracy to frame-based systems (Varma & Eldridge, 2006).
The Neuromate has also been used in epilepsy surgery (Sieradzan, et al., 2013). In many epilepsy surgeries, it is not possible to plan the surgery using non-invasive studies like MRI or PET/CT. Instead intracranial EEG recording is used to identify the seizure onset zone for removal. Robotic intracranial EEG (sEEG - stereotactic implantation of multiple depth electrodes) is a safe technique for performing these measurements. The advantages are: no need for craniotomy and lower risk of infection or complications.

Figure 19: The Neuromate robot being tested for accuracy with a phantom (Source: Varma & Eldridge, P (2006)).

Figure 20: Full view of the Neuromate Robot (Source: Varma & Eldridge, P (2006)).
Horizon 2020
EDEN 2020 is part of a funding program by the EU/EC called Horizon 2020. The programme focusses on 3 main areas: basic science, career development and training of researchers and industrial leadership. This last area covers potential solutions to a number of “societal challenges” in different areas such as health, energy, transport, the environment, security and the bioeconomy. The goal for the societal challenges areas in to encourage the implementation of solutions rather than technology development.
Other Projects
In addition to EDEN2020 there are a number of other Horizon 2020 funded projects in a diverse range of areas. A few are summarised below:
- E-ferry (E-Ferry Partners, 2016) is a project that involves the design, building and demonstration of a fully electrically powered car- and passenger ferry so that the overall emission and pollution caused by waterborne transportation can be reduced in the future.
- sCO2-HeRo (The supercritical CO2 Heat Removal System) (sCO2-HeRo Partners, 2016) – A system for reliably and efficiently removing residual heat from nuclear fuel without the need for external power sources. The system aims to be a backup cooling system for reactor cores in case of power loss. Thereby improving the safety of nuclear reactors.
- ChiLTERN (ChiLTERN, 2016) – The ChiLTERN project aims to improve the level of personalised therapy reveived by children with liver cancer. For example, ensuring that each patient receives the right amount of chemotherapy and undergoes the most appropriate surgical procedures. This will be done by assigning patients more accurately to risk groups using genetic tests and biomarkers. Imaging technology tools for planning liver operations in a safer way will also be explored.
- “Click-It” (Click-It Consortium, 2016) – The “Click-It” project aims to improve the use of nuclear imaging to monitor the delivery of nanomedicines. This is currently difficult because most of the nanomedicines are short lived and so difficult to detect using nuclear medical imaging. If longer lasting isotopes are used then the patient receives an unnecessarily high radiation dose. Click-It will develop new tracers to allow for the monitoring of nanomedicines and will test these in canine patients.
Bibliography
Abrishamkar, S. et al., 2011. A New System for Neuronavigation and Stereotactic Biopsy. J Surg Tech Case Report, Volume 3, pp. 87-90.
Agar, N. Y. et al., 2013. Development of Stereotactic Mass Spectrometry for Brain Tumor Surgery. Neurosurgery, 68(2), pp. 280-290.
Barua, N. U. et al., 2013. Robot-guided convection-enhanced delivery of carboplatin for advanced brainstem glioma. Acta Neurochirurgica, 155(8), pp. 1459-1465.
Bilger, A. C. et al., 2017. P14.20 Local control an overall survival after frameless LINAC radiosurgery: a single center experience. Neuro-Oncology, 19(suppl_3), p. iii106.
Bjartmarz, H. & Rehncrona, S., 2007. Comparison of Accuracy and Precision between Frame-Based and Frameless Stereotactic Navigation for Deep Brain Stimulation Electrode Implantation. Stereotactic and Functional Neurosurgery, Volume 85, pp. 235-242.
Bot, M. et al., 2015. Analysis of Stereotactic Accuracy in Patients Undergoing Deep Brain Stimulation Using Nexframe and the Leksell Frame. Stereotactic and Functional Neurosurgery, Volume 93, pp. 316-325.
Breneman, J. C. et al., 2009. Frameless Image-Guided Intracranial Stereotactic Radiosurgery: Clinical Outcomes for Brain Metastases. International Journal of Radiation Oncology, Biology and Physics, 74(3), pp. 702-706.
ChiLTERN, 2016. Children’s Liver Tumour European Research Network, Brussels: European Comission.
Click-It Consortium, 2016. "In Vivo Click PET Imaging Agents”: Improving clinical companion diagnostics, Brussels: European Comission.
Dammers, R. et al., 2008. Safety and efficacy of frameless and frame-based intracranial biopsy techniques. Acta Neurochirurgica, Volume 150, p. 23.
Dorward, N., Paleologos, T., Alberti, O. & Thomas, D., 2002. The advantages of frameless stereotactic biopsy over frame-based biopsy.. British Jounral of Neurosurgery, 16(2), pp. 110-8.
EDEN2020, 2017. EDEN2020 - Objectives, Approach and Impact. [Online] Available at: http://www.eden2020.eu/about/objectives-approach-and-impact/ [Accessed 11 06 2017].
E-Ferry Partners, 2016. E-ferry Report Summary, Brussels: European Comission.
Fanous, A. A. et al., 2017. Frameless and Maskless Stereotactic Navigation with a Skull-Mounted Tracker. World Neurosurgery, Volume 102, pp. 661-667.
Grove, J., 2011. 'Triple miracle' sees huge rise in EU funds for frontier research. London: The Times Higher Education.
Khan, F.R. and Henderson, J.M., 2013. Deep brain stimulation surgical techniques. Handb Clin Neurol, 116, pp.27-37.
Liu, F., Watts, T. & Rodriguez y Baena, F., 2016. Intraoperative GPU-based Surgical Navigation for Needle Steering. GPU Technology Conference, p. Poster.
Lobão, C. A. F., Nogueira, J., Dutra do Souto, A. A. & Antonio de Oliveira, J., 2009. Cerebral biopsy: comparison between frame-based stereotaxy and neuronavigation in an oncology center. Arquivos de Neuro-Psiquiatria, 67(3b), pp. 876-881.
Liu, F., Watts, T. & Rodriguez y Baena, F., 2016. Intraoperative GPU-based Surgical Navigation for Needle Steering. GPU Technology Conference, p. Poster.
Morsy, A. A. & Ng, W. H., 2015. Awake craniotomy using electromagnetic navigation technology without rigid pin fixation. Journal of Clinical Neuroscience, 22(11), pp. 1827-1829.
Murphy, M. J. & Cox, R. S., 1996. The accuracy of dose localization for an image-guided frameless radiosurgery system. Medical Physics, Volume 23, pp. 2043-2049.
Orringer, D. A., Golby, A. & Jolesz, F., 2012. Neuronavigation in the surgical management of brain tumors: current and future trends. Expert Review of Medical Devices, 9(5), pp. 491-500.
Raabe, A., Krishnan, R., Zimmermann, M. & Seifert, V., 2003. Frame-less and frame-based stereotaxy? How to choose the appropriate procedure. Zentralblatt fur Neurochirurgie, 64(1), pp. 1-5.
Radler, J. R., 1993. Apparatus for and method of performing stereotaxic surgery. United States of America, Patent No. US5207223.
Radler, J. R., 2004. Frameless radiosurgery treatment system and method. United States of America, Patent No. US6778850.
Safaee, M., Burke, J. & McDermott, M. W., 2016. Techniques for the Application of Stereotactic Head Frames Based on a 25-Year Experience. Cureus, 8(3), p. E543.
sCO2-HeRo Partners, 2016. sCO2-HeRo Report Summary, Brussels: European Comission.
Sieradzan, K. et al., 2013. ROBOTIC STEREO EEG IN EPILEPSY SURGERY ASSESSMENT. J Neurol Neurosurg Psychiatry, 84(11), pp. E2-E3.
Smith, J. et al., 2008. Role of extent of resection in the long-term outcome of low-grade hemispheric gliomas.. Journal of Clinical Oncology, 26(8), pp. 1338-45.
Smith, J., Quiñones-Hinojosa, A., Barbaro, N. & McDermott, M., 2005. Frame-based stereotactic biopsy remains an important diagnostic tool with distinct advantages over frameless stereotactic biopsy.. Journal of Neuro-oncology, 73(2), pp. 173-9.
Smith, T. R. et al., 2014. Impact of fiducial arrangement and registration sequence on target accuracy using a phantom frameless stereotactic navigation model.. Journal of Clinical Neuroscience, 21(11), pp. 1976-1980.
Uluç, K., Kujoth, G. C. & Baskaya, M. K., 2009. Operating microscopes: past, present, and future. Journal of Neurosurgery, 27(3), p. E4.
University Hospital Southampton, 2014. Awake craniotomy. [Online]
Available at: http://www.uhs.nhs.uk/OurServices/Brainspineandneuromuscular/Neurosurgery/Diagnosisandtreatment/Braintumours/Awakecraniotomy.aspx
[Accessed 17 06 2017].
Varma, T. R. K. & Eldridge, P., 2006. Use of the NeuroMate stereotactic robot in a frameless mode for functional neurosurgery. THE INTERNATIONAL JOURNAL OF MEDICAL ROBOTICS AND COMPUTER ASSISTED SURGERY, Volume 2, pp. 107-113.
Virdyawan, V., Oldfield, M. & Rodriguez y Baena, F., 2016. Laser Doppler Based Sensing for Blood Vessel Detection with a Steerable Needle. 6th Joint Workshop on New Technologies for Computer/Robot Assisted Surgery, p. Presentation.
Wang, D. et al., 2014. Pain experience using conventional versus angled anterior posts during stereotactic head frame placement for radiosurgery.. Journal of Clinical Neuroscience, 21(9), pp. 1538-42.
West, J. B. et al., 2001. Fiducial Point Placement and the Accuracy of Point-based, Rigid Body Registration. Neurosurgery, 48(4), pp. 810-818.
White, T. et al., 2017. Frameless Stereotactic Insertion of Viewsite Brain Access System with Microscope-Mounted Tracking Device for Resection of Deep Brain Lesions: Technical Report. Cureus, 9(2), p. e1012.
Woerdeman, P. A. et al., 2007. Application accuracy in frameless image-guided neurosurgery: a comparison study of three patient-to-image registration methods. Journal of Neurosurgery, 106(6), pp. 1012-1016.
Malone, Hani R., et al. "Simulation in neurosurgery: a review of computer-based simulation environments and their surgical applications." Neurosurgery 67.4 (2010): 1105-1116.
Waran, Vicknes, et al. "Utility of multimaterial 3D printers in creating models with pathological entities to enhance the training experience of neurosurgeons: technical note." Journal of neurosurgery 120.2 (2014): 489-492.
2 Kommentare
Unbekannter Benutzer (ga67yur) sagt:
20. Juni 2017Really nice wiki. The information is detailed but still easy to read which is good. I especially like that you included several examples for future/current developements. As a side note: your figures are not numbered yet but instead there is a "?". Personally I think it would be nice if you include direct links to your sources, but that's just a matter of taste.
All in all great work!
Unbekannter Benutzer (ga39tec) sagt:
20. Juni 2017Your wiki is very detailed and well written. I like your citation-style, too: it results in a very ordered bibliography. Regarding the order/structure of the article: as you have a lot of detail, subpages would help structuring the article and give a better overview of all covered topics.