Brain Tumor Surgery
After being diagnosed with a brain tumor, there exist many different treatment options that can be applied to try and cure the tumor. A first step in most cases is to surgically remove the tumor in the brain. This procedure often reduces neurological symptoms caused by the mass in the brain and allows the doctors to analyze and correctly classify the tumor.
Pre-surgical considerations
Every neurological operation is of higher risk than ordinary operations, since every mistake during the procedure can have severe consequences, like loss of speech and loss of other brain functions or even death.
To minimize the risk of the operation, every surgery is planned and the patient and tumor are observed and analyzed constantly before the procedure. To achieve a high degree of detail and a considerable amount of information about the underlying medical problem, medical imaging is used. In addition to preoperative diagnosis and planning, those imaging techniques are used during the surgery to help guide the surgeon through the different parts of the brain and help him reach the tumor without injuring the brain.
Besides medical imaging as an important part of the operation, the anesthesia, that allows the doctor to undertake the procedure, plays a big role in surgical preparations. Depending on the type of operation, the anesthesiologist must put the patient in a condition, in which the surgeon can operate without the risk of movement by the patient. In some cases, this means a local anesthesia where the patient is still able to conscious to analyze if any brain functions have been damaged by the surgeon and to ease the navigation in the brain [1].
Surgical Techniques
There exist many different possibilities to operate on a brain tumor, depending on the size, location and abilities of the surgeon. In the following section, we will present the most common procedures.
Craniotomy:
During this operation, the brain is exposed at the location of the tumor, so the doctor can easily access the tumor and remove it. This procedure is often combined with biopsies, radiotherapy or other treatment options for brain tumors. Craniotomies can be categorized by the type and location of the incision.
A bifrontal craniotomy consists of removing the skull bone at the forehead and accessing the front of the brain. Even though the incision is made at the hairline to hide the resulting scar, this type of craniotomy is very invasive. Picture (1)
A similar approach is the orbitozygomatic craniotomy, where the cheek bone is removed to gain access to the brain. Like a bifrontal operation, this procedure is very invasive. Picture (2)
The supraorbital craniotomy begins with an incision at the eyebrow. Like the bifrontal craniotomy, this operation enables the surgeon to remove tumors in the front of the brain. Picture (3) shows the operational steps and the minimal invasive nature of the operation.
A retrosigmoid craniotomy is used to operate on tumors located in the brainstem and the cerebellum. The incision is made behind the ear to achieve minimal invasion.
A translabyrinthine procedure is like the retrosigmoid craniotomy, since in both cases the incision is made behind the ear. After the skin is removed, the mastoid and parts of the inner ear bone are removed to gain access to a tumor near the ear
This type of surgery has a high risk of complications, since part of the brain are exposed for a long time. This risk has brought up less invasive operating techniques [2].



Procedure illustration for bifrontal craniotomy (left) [3] , (2) orbitozygomatic craniotomy (middle) [4], (3) supraorbital craniotomy (right) [5]
Neuroendoscopy:
Neuroendoscopes allow the access to parts of the brain without having to expose a large part of the brain, like when performing craniotomies. In most cases an opening of some centimeters is enough to insert the endoscope. This device can be rigid, flexible or a channel neuroendoscope and are equipped with a small camera and other tools to remove masses from the brain. To introduce the endoscope into the brain, the surgeon uses a sheath. In order to complete the procedure effectively, the whole operation has to be planned beforehand and during the surgery, the placement of the endoscope is monitored by medical imaging. Depending on the location of the tumor and the type of tumor, the MRI or CT imaging method is used. Since the needed opening is very small, the procedure is minimally invasive and allows for a quick recovery of the patient. In contrast to the advantages of this surgery, the risk of complications constant: loss of brain function, cardiac dysrhythmia or other severe problems [1].
Shunt:
A shunt is a tube that is inserted into the brain in order to relieve cranial pressure. This elevated pressure is caused by a surplus of CSF and can lead to cause symptoms like headaches, epilepsy, mood changes. In addition to relieving pressure, the shunt can be expanded to administer medicine directly into the brain. This is an effective way to combine treatment and symptoms relieve of a cancer patient [6].

Placement of a shunt [7]
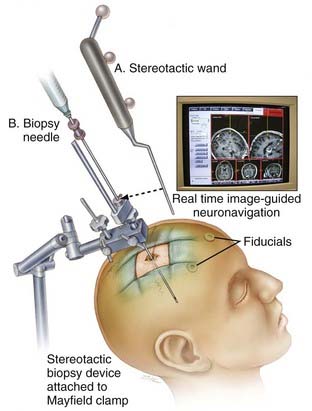
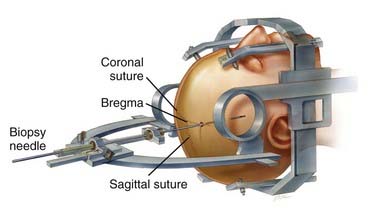
Stereotactic Biopsy:
In some cases, diagnosis and classification of a tumor is only possible by obtaining a physical sample of the mass. This is done by taking a biopsy of the brain tissue that contains the tumor. There exist two possible setups to complete this procedure: frameless biopsy and framed biopsy.
- Frameless biopsies are easier and quicker to perform, but they are not as accurate as framed biopsies
- Framed biopsies are very accurate, but require more precision when setting up the procedure.
In both cases, the whole procedure has to be planned beforehand with up to date imaging of the brain to get the accurate position of the tumor and calculate the shortest way to the area [1].


standard set up for biopsies, frameless biopsy (left) [8], framed biopsy (right) [9]
Treating Gliomas Surgically
The glioma is one of the most common brain tumors, but there are many others like meningioma, lymphoma. In this chapter we will concentrate on gliomas because of their high number of occurrences and high number of possible operations.
Gliomas:
A tumor can be classified in four different classes that reflect the severity of the tumor. In evaluating the possible treatment options, the grade of a tumor plays a big role to determine if a surgery is recommendable. With the evolution of medical imaging, low-grade gliomas are being detected at early stages. This is good because treatment for cancer can be administered very early and in conclusion elevate the survival rate of patients.
Depending on the detected tumor, different treatments are recommended:
- If the detected tumor is very large, surgery is in most cases not recommended, since it is very difficult resect the entire cancer cells. Often debulking the tumor is only done to reduce intracranial pressure and ease the symptoms caused by this high pressure. If the pressure is normal, it has not been proven that removing the tumor is helping to cure the patient.
- A small glioma in its early stages is only operated after evaluation of the different brain scans. To remove such a tumor, the accurate location of the mass must be determined and the path to reach it has to be planned. This scenario is the minority of cases.\
- Is the detected tumor not accurately detectable or diagnosable, the surgeon and patient have to carefully weigh the risk of undergoing a craniotomy. Not only the experience of the doctors play a major role in the decision-making process, but also the different alternative treatment options like chemotherapy or steroids.
Low-grade gliomas are often located deep in the white matter of the brain, which makes it very hard to operate them. This explains why operable gliomas constitute the minority of glioma diagnosis. Since most of these tumors are located in white matter and are difficult to reach, operations have to be performed as an awake craniotomy. This allows the surgical team to check if any parts of the brain have been damaged by the actions of the surgeon. Such an operation needs special anesthetic to numb the brain but still allow the patient to be awake.
Video glioblastoma [10]
A high-grade glioma is often malignant and very aggressive, which means a surgery to remove such a tumor has a low possibility of resecting all the cancer cells. This means that the cancer is likely to reemerge after the surgery. A case to case evaluation of the medical situation has to be done for each case. Often to determine the grade of the detected tumor, a biopsy must be done on the tumor. In the same time, a resection can be done to remove the mass directly without accurately diagnosing it before the operation. All those factors have to be considered after a high-grade glioma has been detected in a patient [1].
Radiation Therapy
Radiation therapy is one of the techniques for treating brain cancers. This technique uses high energy x-rays (in some cases gamma rays, protons), concentration of x-rays in one particular area to destroy cancer cells. As a consequence, the radiated area should not be broadly spread in the body and usually in small to moderate sizes. This technique is also knows as radiotherapy or x-ray therapy. The success of radiation therapy for cancer treatments relies on the possibility to destroy the DNA of cancer cells. The main task of radiation is to damage the DNA of cancer cells, which afterwards stop dividing and spreading, consequently die. However, through radiation therapy, the patient is prone to destroying healthy cells as well. Nevertheless, taking into consideration the advantages and disadvantages of this process, the differences are inconsiderable. In regards to Brain tumors, a radiation therapy is given in order to destroy a cancerous mass in the brain or spinal cord, in order to prevent a recurrence of a tumor, or both [11][12].
Before starting with a radiation therapy, there is a lot of planning involved. The person in charge of planning the procedure is the Radiation Oncologist. Firstly, the radiation oncologist preforms several images and scans the tumor area together with its surrounding. After the precise shape, size and location of the tumor is identified, it is essential for the patient to lay in the exact same position every time the procedure is carried. Since radiation therapy is usually given is several treatments, in order to make sure that the position of the body (head) is exactly the same after each treatment, different Head Masks, temporary skin marks or sometimes tattoos help for this alignment. After this step, the Radiation Oncologist calculates the dose of radiation to be given depending on the tumor size, position and number of treatments. These calculations take into consideration the dose to destroy cancer cells and minimally damage the surrounding of the tumor. Because of the severity of x-rays, it is very likely that after one treatment with radiation therapy, the patient is not allowed to receive another treatment in the same area after a tumor recurrence [12].


Brain tumor treatment mask through radiation therapy (left) and radiation planning (right) [13][14]
According to cancer.org, there are three different methods of radiation therapy:
- External Radiation Therapy
- Internal Radiation Therapy (brachytherapy)
- Systemic Radiation Therapy
External Radiation Therapy
External Radiation Therapy is one of the most commonly used methods today. This method consists of a machine that uses high energy rays (beams) from outside the body, pointing towards the tumor. In many sources this machine is found as a Linear Accelerator or “Linac”. The most recent radiation therapy machines are very precise and are focused through very powerful computers, which allow the oncologists to use higher doses, since the “only” main target is the tumor itself [15].
External Radiation therapy is mainly conducted at a hospital or treatment center, under the supervision of the radiation oncologist. Before the procedure starts, the radiation oncologists preform a procedure called the “simulation” which basically is to pinpoint exactly the location of the tumor, size and shape. After the simulation, the total dose of external radiations is calculated and divided into fractions. The fractioning of the therapy is done because of the damaging effects of giving the whole dose at a time to the normal cells would be unrecoverable. Normally, a fraction of the total dose is given to the patient daily from Monday to Friday, from 5 to 8 weeks in repetition, having the weekend free for normal cell recovery. The exact number of fractions and total dose is calculated based one the following factors:
- Size and tumor location
- Type of cancer
- General health condition

External Radiation therapy for brain tumor [16]
External Radiation therapy is very straight forward procedure. It does not make the patient feel pain, it is similar to getting an x-ray. However, it is a bit longer, between 30 to 45 mins because of the positioning of the patient and the hardware. Other parts of the body that are not being treated are shielded in order to avoid radiation [15].
There are several external radiation therapy techniques used which include:
- Three-dimensional conformal radiation therapy (3D-CRT)
- Image guided radiation therapy (IGRT)
- Intensity modulated radiation therapy (IMRT)
- Helical-tomotherapy
- Proton beam radiation therapy
- Stereotactic radiosurgery
- Intraoperative radiation therapy (IORT)
Internal Radiation Therapy (brachytherapy)
This type of Radiation Therapy is not very likely to be applied in brain tumors, however it is one of the radiation therapy methods used nowadays. Internal Radiation therapy in the literature is also known as Brachytherapy, where a radioactive implant is put inside the body of the patient near the tumor, the implant irradiates for a period of time to destroy the tumor. Depending on the results from the planning procedure, the patient either gets a permanent or temporary implant. Brachytherapy allows higher doses to be given over a shorter period of time, over a smaller area. This is the main advantage over the External Radiation therapy [17].
The implant is usually put into the patient within very isolated surgery rooms, in order to keep the radiation localized. The procedure is preformed either through local or general anesthesia. Depending on the type of Brachytherapy given, the implant gets to stay within the patient from few minutes or days, to forever. There are two parts of the procedure, the first part is the applicator, which is a mechanism used to ease the process of putting the radioactive material (second part) to place. In case high-energy doses are used, the applicator is left in place, only the radioactive material is replaced. Since a radioactive material is implanted in the patient’s body, this means that the patient emits radioactive rays, hence, they might be isolated or not allowed in proximity of other people [17].
Systemic Radiation Therapy
Systemic Radiation therapy it is not very likely to be given for brain tumors, as far as the literature is concerned, it is mainly for thyroid, bone, and prostate cancer. This type of therapy uses a radiopharmaceutical drug (radioactive substance), in the form of liquid, which is taken either orally or intravenously. The antibodies in the liquid attach to cancer cells and irradiate to damage the tumor mass. Some examples of Radiopharmaceuticals include iodine, strontium, samarium, and radium. Same as the Brachytherapy, Systemic Radiation irradiates from inside the body and hence the patient is at a level radioactive. Thus, it is suggested to stay isolated for the days the therapy is given, and very strict rules apply for normal daily activities, such as using the toilet, daily water consumption and outside visits [18].
Stereotactic Radiotherapy
Stereotactic Radiotherapy (SRT) falls within the external radiotherapies and it is one of the most important and commonly used therapies given for brain tumors. This technique uses computers and scanners to produce very accurate 3D models of the brain (together with the tumor), and precisely know the shape, size and position of the tumor. After, many small beams are directed towards the tumor, from different angles, adding up the total dose to create a high focused overlap of beams to destroy the tumor. This way, the damage to healthy cells in the neighborhood of the tumor is significantly lower compared to conventional external treatment [19].

Stereotactic Radiotherapy planning and angle of beams [20]
Another very sophisticated technique is called Stereotactic Radiosurgery (SRS) which is given within one dose to destroy the tumor. However, these techniques are usually used in smaller tumors (according to thebraintumorcharity.org, for tumors less then 3cm at the widest part), assuming the same high dose of radiation is given equally in all parts of the tumor. Compared to external radiation therapy, in SRT a mask or head frame is a must. Because of the accuracy needed, there is no room for any mistake in even small fractions of mm [19].
Radiation Therapy Side Effects
Beside the radiation harm towards healthy cells, there are considered some other side-effects from radiation therapy. Even though it varies on patients, tumor sizes and other factors, some general expected side-effects are to be considered. One commonly side effect from brain tumor treatment is hair loss. However, it is not a complete hair loss, but it happens in patches, only in the parts where the beam hits the skull. Tiredness is another side-effect which happens to patients, and lack of energy. It is suggested to sleep more and have rests after treatments. Because of the swellings that might happen in the brain in the affected area, the symptoms might get worse while in treatment, however, this is completely normal and usually doctors prescribe steroids to prevent from happening [21].
Chemotherapy
Chemotherapy is another very common method to treat brain tumors. Chemotherapy uses drugs to destroy cancer cells, and it is given either on its own or alongside with radiotherapy. Usually is used to destroy, stop the growth of a tumor before surgery, however it is also used after the surgery to prevent recursion. Chemotherapy makes use of cytotoxis (anti-cancer) drugs which affect the growth of tumor cells and the way they replicate, intended to lead to cell death. However, chemotherapy affects the whole body (in other words all cells), but the cancerous cells have difficulties on recovering compared to healthy cells. Nevertheless, there are difficulties that the drugs always reach the brain because of the blood-brain barrier. In such cases, there are also methods that the drugs are directly injected in the cerebrospinal fluid [22][23].
Even though still on research, there are a lot of drugs that are filtered out from the blood-brain barrier, and do not have the desired effect on the tumor. Still, there are few techniques to bypass the blood-brain barrier to deliver the drugs in particular parts of the brain. Although still not a standard procedure, there is a way to temporarily open the blood-brain barrier and successfully deliver the drugs in the brain. The drug “Mannitol” is used to temporarily open the blood-brain barrier and high doses of drugs pass into the brain injected from an artery or vein. The blood-brain barrier returns to its normality as the effect of Mannitol expires [22].
Chemotherapy is given in series of treatments, followed by resting periods, all together called a cycle. For brain tumors, the course of treatment lasts from 3 to 6 months consisting of 4 to 8 cycles. Each cycle consists of few weeks of treatment, followed by a resting period to give time to the body to recover. Each treatment is conducted under the supervision of professionals in hospitals or treatment centers. The drugs are delivered through tablets, or injection. For intravenous treatment, which is the most common case for brain tumors, the patient stays at hospital from 30 mins to few hours until the drugs designated for that treatment are delivered [23][24].
Because of the effects of the drugs to the whole body, patients are expected to have lower immunity, increased risk from bleeding, tiredness, nausea, hair loss, change in taste and many other side effects. Some of the side effects are expected to come on and off depending on the cycle (treatment – rest period interval). The side effects are to go away once the treatment has been complete. Upon completion, the patient undergoes further scans to make sure the treatment has been successful, and regular check-up appointments are scheduled to keep the development of the tumor under supervision [24][25].
Targeted and Immunotherapy
Current studies show that beside the standard procedures such as surgery, radiation therapy and chemotherapy, a very promising strategy is targeted therapies and immunotherapy against brain cancer. Making use of the immune system against cancer is very quickly becoming a leading strategy for treating tumors. So far, this kind of strategy has been very successful for blood cancers, however, a study done in a patient with advanced recurred brain cancer showed to be very successful. This patient with Glioblastoma, a very aggressive brain cancer, who has already been treated with surgery and radiation, despite the treatment the cancer recurred and spread to other parts of the brain. After the immune cells have been extracted from the patient, they have been reengineered to recognize and destroy “Glioblastoma” tumor cells. Upon removal of the tumor, these reengineered cells are applied in the area and the tumor stopped growing [26][27].
One targeted treatment for brain tumors is called the drug “Bevacizumab” given intravenously, which stops the formation of new vessels around the tumor. Tumor cells have the characteristic of huge energy consumptions and uncontrolled cell reproduction, which functions cannot live properly without a steady blood flow provided through blood vessels, hence, the cancer cells start to malfunction and gradually die. This process stops the tumor growth, and in literature is known as Angiogenesis. Thus, unlike chemotherapy that has an effect on all cells in the body, targeted therapy uses the information from the DNA of cancer cells in order to specifically destroy those cells, hence, avoiding damaging healthy cells as well as few other side effects [27].
Steroids
Steroids have been administered to brain tumour patients for several decades now and are still widely used today, despite known side effects and unclear action mechanism. They reduce swelling (edema) and posses and anti inflammatory effect and are therefore often administered before, during, and after surgery. However, they also have severe side effect. The most prominent ones are:
- Gastrointestinal bleeding (prophylactic use of stomach protecting drugs is common)
- Myopathy (muscle weakness)
- infections
- osteoporosis (becomes a problem once survival rates increase)
- mood disturbance
Furthermore, the exact mechanisms of action of corticosteroids is still poorly known to date. It is suspected, that they may interfere with the treatment of the tumour by influencing the properties of the tumour cells as well as the neuronal progenitor cells. New therapeutic agents to reduce swelling have been developed, which could soon limit the use of glucocorticoides in brain tumour therapy[28].
Current clinical studies
Various clinical trials investigating different combinations of drugs and therapy approaches can be found in the literature, each of them addressing different aspects of the obstacles present, when it comes to effective brain tumour treatment. In the following some of the current studies will be discussed briefly.
Tumor Treating Fields – A treatment approach in clinical trial phase III
In addition to surgery, radiotherapy and chemotherapy a new treatment approach has now entered clinical research phase III. This new technology is called Tumour Treating Fields. The approach is to apply alternating, low-intensity, intermediate frequency electric fields to the tumour which is supposed to disrupt cell division and tumour growth [29][30][31].
The method is supposed to disrupt cell division on different stages and thus ultimately leading to cell death of the fast growing tumour cells.
- Prevent the formation of microtubuli which drive to the separation of the chromatids.
- Induce an imbalanced/erroneous distribution of the chromatids.
- Create a gravitational centre at the cleavage site of the daughter cells.



Meta-, Ana- and Telophase of the cellddivision under the force of the electic field, which is indicated by the white lines. An alternating orthogonal field shall allow disruption of as many cell divisions as possible [32].
The leading research facility is a company called "novocure" which delivers their product "Optune", a device consisting of electrodes that are placed onto the skull and deliver the aforementioned electric field. Should this method be successful, it would mean a great improvement of the quality of life for many brain tumour patients, since it would avoid the use of the more bothersome traditional approaches, which have severe side effects.
Several publications can be found on TTF in clinical trials, however the "most relevant" articles according to Google scholar, are all (co-)authored by scientist somehow affiliated to "novocure" or received funding from this company, so there is still need for an independent assessment of the method[29][30][31][33].
Convection-enhanced delivery
One of the main problems in treating brain tumours is bypassing the blood-brain barrier, and thus the effective delivery of chemotherapy. Convection-enhanced delivery aims to bypass this obstacle. The idea is to insert a sort of cannula into the tumour and deliver the tumour treating agents via a syringe. The pressure one can exert via the needle is supposed to increase the distribution of the drug through the tumour. The placement of the needle inside the tumour could greatly decrease the concentration of the toxic drug necessary in comparison to diffusion based methods. Trials have been conducted using various treatments. However in practice several challenges present itself, such as the cannula design and placement and reflux of the medication, as well as cost of the procedure and choice of the optimal drug [34].

Illustration of the principle of convection-enhanced delivery and the distribution of the drug within the tumor (left). On the right a scenario considering the reflux is shown [34].
Tumour metabolomics
It is know, that tumour cells have an altered metabolism relying mainly on glycolysis for energy generation. In epilepsy studies a low glucose and high fat diet (ketogenic diet -- KD) has been implemented as a treatment approach. Studies suggest, that a special diet, such as KD could have beneficial effects on the therapy outcome of brain tumours due to their altered metabolism, however clinical trials to further investigate the field will be necessary [35].
References
Moore, Anne J.; Newell, David W.: “Tumor Neurosurgery, Principles and Practice”, Springer, ISBN: 978-1-84628-291-1
“Craniotomy” [Online] Available: http://www.hopkinsmedicine.org/healthlibrary/test_procedures/neurological/craniotomy_92,P08767/. [Accessed: 21-May-2017]
- "bifrontal craniotomy" [Online] Available: http://www.anatomicaljustice.com/dpic/bifrontal_craniotomy_1.jp [Accessed: 21-May-2017]
- "orbitozygomatic craniotomy" [Online] Available: https://www.barrowneuro.org/assets/Figure-8.-Steps-involved-in-the-orbitozygomatic-approach..jp [Accessed: 21-May-2017]
- "subortbital craniotomy" [Online] Available: https://www.degruyter.com/view/j/ins.2013.1.issue-2/ins-2013-0010/graphic/ins-2013-0010_fig2.jpg [Accessed: 21-May-2017]
“Shunt Procedure” [Online] Available: http://www.hopkinsmedicine.org/neurology_neurosurgery/centers_clinics/cerebral-fluid/procedures/shunts.html. [Accessed: 21-May-2017]
" Shunt Diagram" [Online] Available: https://upload.wikimedia.org/wikipedia/commons/thumb/c/c7/Diagram_showing_a_brain_shunt_CRUK_052.svg/280px-Diagram_showing_a_brain_shunt_CRUK_052.svg.png [Accessed: 21-May-2017]
- " frameless biopsy" [Online] Available: https://clinicalgate.com/wp-content/uploads/2015/03/B9781416053163001179_f114-003-97814160531633.jpg [Accessed: 21-May-2017]
- "framed biopsy" [Online] Available: https://clinicalgate.com/wp-content/uploads/2015/03/B9781416053163001179_f114-001-97814160531636.jpg [Accessed: 21-May-2017]
“Brain Tumor Surgery: Surgical removal of glioblastoma” [Online] Available: https://www.youtube.com/watch?v=VXcZOjl9C48 [Accessed: 21-May-2017]
- American Cancer Society, "Radiation Therapy Basics," American Cancer Society, February 2017. [Online] Available: https://www.cancer.org/treatment/treatments-and-side-effects/treatment-types/radiation/radiation-therapy-guide/what-is-radiation-therapy.html [Accessed: 23-May-2017]
- National Cancer Institute, "Radiation Therapy for Cancer," National Cancer Institute, June 2010. [Online] Available: https://www.cancer.gov/about-cancer/treatment/types/radiation-therapy/radiation-fact-sheet [Accessed: 23-May-2017]
- Brain Tumor Treatment Image [Online] Available: http://haf9jn6not-flywheel.netdna-ssl.com/wp-content/uploads/2016/04/radiation-therapy-stem-cells-604x270.jpg [Accessed: 23-May-2017]
- Brain Tumor Treatment Planning Image [Online] Available: http://www.mygenesishealth.com/treatment-options/radiation-oncology/images/imrt-brain-cancer.jpg [Accessed: 23-May-2017]
- American Cancer Society, "External Beam Radiation Therapy," American Cancer Society, February 2017. [Online] Available: https://www.cancer.org/treatment/treatments-and-side-effects/treatment-types/radiation/radiation-therapy-guide/external-radiation-therapy.html [Accessed: 23-May-2017]
- External Beam Radiation Therapy Image [Online] Available: http://www.medicalnewstoday.com/content/images/articles/282/282760/man-undergoing-external-beam-radiotherapy.jpg [Accessed: 23-May-2017]
- American Cancer Society, "Internal Radiation Therapy (Brachytherapy)," American Cancer Society, February 2017. [Online] Available: https://www.cancer.org/treatment/treatments-and-side-effects/treatment-types/radiation/radiation-therapy-guide/internal-radiation-therapy.html [Accessed: 23-May-2017]
- American Cancer Society, "Systemic Radiation Therapy," American Cancer Society, February 2017. [Online] Available: https://www.cancer.org/treatment/treatments-and-side-effects/treatment-types/radiation/radiation-therapy-guide/systemic-radiation.html [Accessed: 23-May-2017]
- The Brain Tumor Charity, "Stereotactic radiotherapy," The Brain Tumor Charity, April 2016. [Online] Available: https://www.thebraintumourcharity.org/understanding-brain-tumours/treating-brain-tumours/adult-treatments/stereotactic-radiotherapy/
- Stereotactic Radiotherapy Planning Image [Online] Available: https://bgsglobalhospitals.files.wordpress.com/2015/06/picture-2-blog.png [Accessed: 23-May-2017]
- Cancer Research UK, "Side effects of radiotherapy," Cancer Research UK, October 2015. [Online] Available: http://about-cancer.cancerresearchuk.org/about-cancer/brain-tumours/treatment/radiotherapy/side-effects [Accessed: 23-May-2017]
- American Brain Tumor Association, "Chemotherapy," American Brain Tumor Association, 2016. [Online] Available: http://www.abta.org/secure/chemotherapy.pdf [Accessed: 23-May-2017]
- The Brain Tumor Charity, "Chemotherapy (adults)," The Brain Tumor Charity, May 2014. [Online] Available: https://www.thebraintumourcharity.org/understanding-brain-tumours/treating-brain-tumours/adult-treatments/chemotherapy/ [Accessed: 23-May-2017]
- American Cancer Society, "Chemotherapy for Adult Brain and Spinal Cord Tumors," American Cancer Society, January 2016. [Online] Available: - https://www.cancer.org/cancer/brain-spinal-cord-tumors-adults/treating/chemotherapy.html [Accessed: 23-May-2017]
- Center Treatment Centers of America, "Chemotherapy for brain cancer," Center Treatment Centers of America, 2016. [Online] Available: http://www.cancercenter.com/brain-cancer/chemotherapy/ [Accessed: 23-May-2017]
- Alice Park, "Experimental Brain Cancer Treatment Is a Success," Time Health, December 2016. [Online] Available: http://time.com/4618566/brain-cancer-treatment-immunotherapy/ [Accessed: 23-May-2017]
Center Treatment Centers of America, "Targeted Therapy," Center Treatment Centers of America, 2016. [Online] Available: http://www.cancercenter.com/treatments/targeted-therapies/ [Accessed: 23-May-2017]
- J. Dietrich, K. Rao, S. Pastorino, and S. Kesari, “Corticosteroids in brain cancer patients: benefits and pitfalls,” Expert Rev Clin Pharmacol, vol. 4, no. 2, pp. 233–242, Mar. 2011.
E. D. Kirson et al., “Alternating electric fields arrest cell proliferation in animal tumor models and human brain tumors,” PNAS, vol. 104, no. 24, pp. 10152–10157, Dec. 2007.
A. M. Rulseh et al., “Long-term survival of patients suffering from glioblastoma multiforme treated with tumor-treating fields,” World Journal of Surgical Oncology, vol. 10, p. 220, 2012.
A. F. Hottinger, P. Pacheco, and R. Stupp, “Tumor treating fields: a novel treatment modality and its use in brain tumors,” Neuro Oncol, vol. 18, no. 10, pp. 1338–1349, Oct. 2016.
- https://www.optune.com/hcp/therapy/moa
- https://www.novocure.com/leadership/
- A. Jahangiri, A. T. Chin, P. M. Flanigan, R. Chen, K. Bankiewicz, and M. K. Aghi, “Convection-enhanced delivery in glioblastoma: a review of preclinical and clinical studies,” Journal of Neurosurgery, vol. 126, no. 1, pp. 191–200, Jan. 2017.
- E. C. Woolf, N. Syed, and A. C. Scheck, “Tumor Metabolism, the Ketogenic Diet and β-Hydroxybutyrate: Novel Approaches to Adjuvant Brain Tumor Therapy,” Front Mol Neurosci, vol. 9, Nov. 2016.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}