An approach to navigation in neurosurgery relies on frame-based and frameless techniques. Both are used to target structures onto an human head with the 3D-coordinates acquired from preoperative imaging.Therefore the relationship between the coordinate space for the preoperative images and that for the surgical field must be calculated. Frame-Based systems use the same frame for preoperative images and the surgery where the relationship of the two coordinate systems is known. In frameless systems point-pair registration or surface contour registration can be used. This frame principle is also as stereotactic radiation therapy explained in Radiation Therapy. This chapter covers both methods and in the end compares them.
Frame-Based Navigation
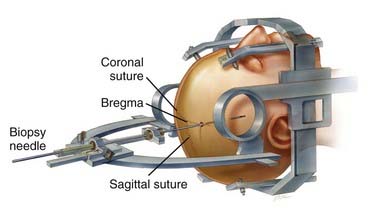
A light weight frame is attached to the patients head using local anesthesia. Now with the help of the frame the surgical instruments can be placed exactly onto the right 3D-Coordinates.
There are several geometric principles on whicht stereotactic systems have been designed though the most common one is the arc radius system serving as the basis for the leksell frame. Here the frame is rigidly attached to the patient’s head to which the semicircular arc is mounted by pivoting shafts that in turn are connected to the graduated bars of the frame. Ultimately, the arc can be manipulated for vertical and anterior-posterior adjustments to permit differential targeting by moving the center of the arc.
Frame-Based system have long been considered "the gold standard for sampling intracranial lesions" though it comes with several limitations:
- attachment of the frame to the patient’s skull often needs to be done on the same day as the operation, which prolongs the surgical time
- posterior fossa lesions are difficult to target
- the frame is bulky and can limit the access to the surigcal field
- maneuvering the frame can be unwieldy
risk of postoperative infection at the frame's fixture points.
Leksell Frame mounted onto a patients head [Source]
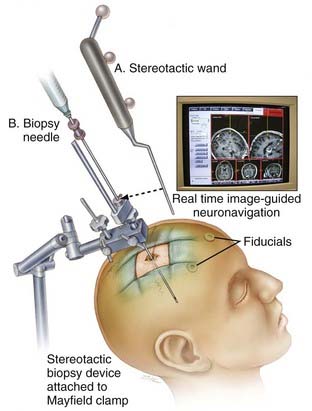
A frameless stereotactic system used for biopsy [Source]
Frameless Navigation
Frameless stereotactic systems were introduced in the 1980s and have been developed since. One thing all systems have in common is that they have to define points in the image and the patient in order to map these two groups to each other. As previously mentioned there are two main techniques used which are Point-Pair Registration and Surface Contour Registration.
Surface-Contour Registration
Surface-Contour registration can e.g. be used by scanning a surface with laser registration and fitting it to a surface model from contours of the patient's head. However compared to point-pair registration it is less accurate.
Point-Pair Registration
Point-Pair matching has been the most common and accurate method to achieve transformation between the two coordinate systems.This method requires a set of at least three non-colinear points to be defined in the coordinates of the images. It has been found that four points are more accurate, however adding more points does no longer increase the accuracy. These points are known as fiducial points and can consist of either natural anatomic landmarks skin-applied markers, or bone-implanted markers. These same fiducial points are defined again within the coordinate system of the surgical field in the operating room. Software is then used to establish the relationship between the coordinates of the fiducial points in the image space and their counterpart in the surgical space
Different systems are used to track the fiducial markers including computer vision and magnetic systems. There is the possibility to use acoustic systems, however the require complex corretion and are susceptible to interference. Optical Systems have the disadavantage that they always require a line of sight. Magnetic systems do not need to see anything but can be disturbed by metallic objects in the operating room. Since optimal placement of this markers can be crucial [6] developed an genetic algorithm to calculate optimal positions of the marker in order to minimize the target registration error. The correspoding marker positions are then shown to the surgeons on the 3D model to help in placement of them.
Comparison
[2] concluded that there is no difference in accuracy using frameless and frame-based markers. However the more recent study [1] suggests that there is a difference, though it is not that big. Both papers recommend to the surgeon to use the method he is most comfortable with.

Comparison of frame-based and frame-less techniques with regard to the diagnostic yield of the biopsy [Source]
There is currently research going on that tries to combine both approaches as suggested in [3]. They propose a head-mounted robot-guided approach that combines the stability of a bone-mounted setup with the flexibility and tolerability of a frameless system. By reducing human interference e.g. manual parameter settings this technology might be particularly useful in neurosurgical interventions that necessitate multiple trajectories.
Bibliography
- Yi Lu et. al. "Comparative Effectiveness of Frame-based, Frameless and Intraoperative MRI Guided Brain Biopsy Techniques" available here
- Dammers R et. al. "Safety and efficacy of frameless and frame-based intracranial biopsy techniques" available here
- F. Grimm et. al. "Blurring the boundaries between frame-based and frameless stereotaxy: feasibility study for brain biopsies performed with the used of a head-mounted robot" available here.
- https://clinicalgate.com/frame-and-frameless-stereotactic-brain-biopsy/#f0020
- http://what-when-how.com/stereotactic-and-functional-neurosurgery/frameless-stereotactic-systems-general-considerations/
- http://medicaldevices.asmedigitalcollection.asme.org/article.aspx?articleid=1451820