This page was written by us to give a brief idea about some basics of human brain anatomy. Of course we can't say that this page is comprehensive, but it can serve as a first step on a way of studying brain tumors for medical imaging purposes. We will not go deep into details, but try to give enough understanding for reading images of different modalities considering brain.

Brain
Basic parts of the brain
The central nervous system (defined as the brain and spinal cord) is usually considered to have seven basic parts: the spinal cord, the medulla, the pons, the cerebellum, the midbrain, the diencephalon, and the cerebral hemispheres. Running through all of these subdivisons are fluid-filled spaces called ventricles. Variations in the shape and size of the mature ventricular space are characteristic of each adult brain region. The medulla, pons, and midbrain are collectively called the brainstem and they surround the 4th ventricle (medulla and pons) and cerebral aqueduct (midbrain). The diencephalon and cerebral hemispheres are collectively called the forebrain, and they enclose the 3rd and lateral ventricles, respectively.


There are several anatomical subdivisions of the forebrain. The most obvious anatomical structures are the prominent cerebral hemispheres. In humans, the cerebral hemispheres (the outermost portions of which are continuous, highly folded sheets of cortex) are proportionally larger than in any other mammal, and are characterized by the gyri (singular, gyrus) or crests of folded cortical tissue, and sulci (singular, sulcus) the grooves that divide gyri from one another (as pictured on the cover of this book, for example). Although gyral and sulcal patterns vary from individual to individual, there are some fairly consistent landmarks that help divide the hemispheres into four lobes.
The most prominent of these is the collection of deep structures involved in motor and cognitive processes collectively referred to as the basal ganglia. Other particularly important structures are the hippocampus and amygdala in the temporal lobes (these are vital substrates for memory and emotional behavior, respectively), and the olfactory bulbs (the central stations for processing chemosensory information arising from receptor neurons in the nasal cavity) on the anterior–inferior aspect of the frontal lobes. Finally, the thalamus lies in the diencephalon and is a critical relay for sensory information (although it has many other functions as well); the hypothalamus, which as the name implies lies below the thalamus, is the central organizing structure for the regulation of the body’s many homeostatic functions (e.g., feeding, drinking, thermoregulation).[0]
The diencephalon consists of :


The lobes
The names of the lobes are derived from the cranial bones that overlie them: occipital, temporal, parietal, and frontal
Frontal lobe
The frontal lobe is separated from the parietal lobe by a space called the central sulcus, and from the temporal lobe by the lateral sulcus. It is responsible for higher executive functions including emotional regulation, planning, reasoning and problem solving. The frontal lobe also contains the primary motor cortex, the major region responsible for voluntary movement.
Parietal lobe
The parietal lobe is behind the frontal lobe, separated by the central sulcus. Areas in the parietal lobe are responsible for integrating sensory information, including touch, temperature, pressure and pain.
Because of the processing that occurs in the parietal lobe, we are able to, for example, discern from touch alone that two objects touching the skin at nearby points are distinct, rather than one object. This process is called two-point discrimination. Different areas of the body have more sensory receptors, and so are more sensitive than others in discerning distinct points.


Temporal lobe
Separated from the frontal lobe by the lateral fissure, the temporal lobe also contains regions dedicated to processing sensory information, particularly important for hearing, recognizing language, and forming memories.
Auditory information
The temporal lobe contains the primary auditory cortex, which receives auditory information from the ears and secondary areas, and processes the information so we understand what we’re hearing (e.g. words, laughing, a baby crying).
Visual processing
Certain areas in the temporal lobe make sense of complex visual information including faces and scenes.
Memory
The medial (closer to the middle of the brain) temporal lobe contains the hippocampus, a region of the brain important for memory, learning and emotions.
Occipital lobe
The occipital lobe is the major visual processing center in the brain. The primary visual cortex, also known as V1, receives visual information from the eyes. This information is relayed to several secondary visual processing areas, which interpret depth, distance, location and the identity of seen objects.[6]
Protection for the Brain
The brain is protected from injury by the skull, meninges, CSF (cerebrospinal fluid) and the blood-brain barrier.
Meninges
The function of the meninges is to cover and protect the brain itself. It encloses and protects the vessels that supply the brain and contains CSF between the pia mater and arachnoid maters. Immediately deep to the periosteum is the periosteal and meningeal which create the dura mater. The dura mater is found all around the brain and its 2 layers separate and create spaces called dural sinuses. See the blue triangle below? The meningeal separates from the periosteal and goes down into the longitudinal fissure. The space that is firmed is a sinus.

Deep to the dura mater is the potential subdural space and deep to that is the arachnoid mater and it’s named arachnoid because of its spider-leggy appearance. Deep to the arachnoid mater is the potential subarachnoid space. Our deepest layer is the pia mater which is a very delicate connective tissue. It literally means “soft mother” as opposed to dura mater which means “durable mother.” [2]
CSF and the ventricular system of the brain
The ventricular system is a set of communicating cavities within the brain. These structures are responsible for the production, transport and removal of cerebrospinal fluid, which bathes the central nervous system.
Cerebrospinal fluid is an ultrafiltrate of plasma that surrounds the brain and spinal cord.
It serves three main functions:
- Protection – It acts as a cushion for the brain, limiting neural damage in cranial injuries.
- Buoyancy – By being immersed in CSF, the net weight of the brain is reduced to approximately 25 grams. This prevents excessive pressure on the base of the brain.
- Chemical stability – The CSF creates an environment to allow for proper functioning of the brain, e.g. maintaining low extracellular K+ for synaptic transmission.

In total, there are four ventricles; right and left lateral ventricles, third ventricle and fourth ventricle.
Lateral Ventricles
The left and right lateral ventricles are located within their respective hemispheres of the cerebrum. They have ‘horns’ which project into the frontal, occipital and temporal lobes. The volume of the lateral ventricles increases with age.
Third Ventricle
The lateral ventricles are connected to the third ventricle by the foramen of Monro. The third ventricle is situated in between the right and the left thalamus. The anterior surface of the ventricle contains two protrusions:
- Supra-optic recess – located above the optic chiasm.
- Infundibular recess – located above the optic stalk.
Fourth Ventricle
The fourth ventricle is the last in the system – it receives CSF from the third ventricle via the cerebral aqueduct. It lies within the brainstem, at the junction between the pons and medulla oblongata.
From the 4th ventricle, the fluid drains into two places:
- Central spinal canal – Baths the spinal cord
- Subarachnoid cisterns – Baths the brain, between arachnoid mater and pia mater. Here the CSF is reabsorbed back into the circulation.[1]
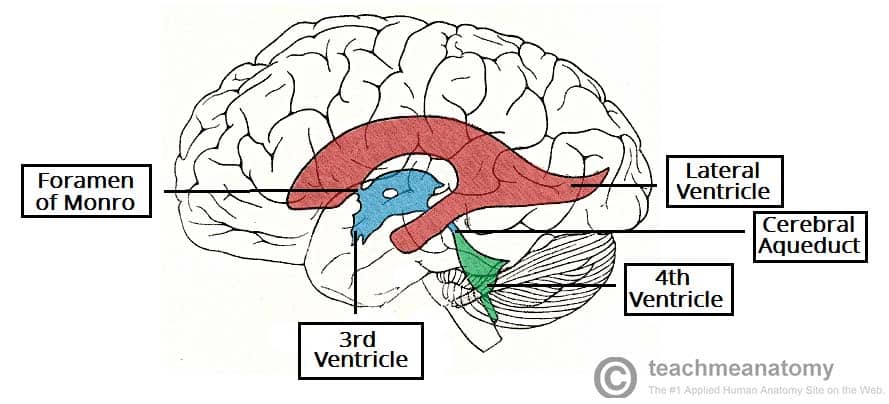
The anatomical positioning of the ventricles of the brain.
Blood-brain barrier
The blood-brain barrier (BBB) protects the neural tissue from variations in blood composition and toxins or pathogens that could cause brain infections. Elsewhere in the body the extracellular concentrations of hormones, amino acids and potassium undergo frequent fluctuations, especially after meals, exercise or stressful times. Since many of these molecules regulate neuronal excitability, a similar change in the composition of interstitial fluid in the CNS can lead to uncontrolled brain activity. The endothelial cells forming the blood-brain barrier are highly specialized to allow precise control over the substances that enter or leave the brain.[4]
Discovery of blood-brain barrier. The discovery of the BBB dates back more than 100 years when, in the 1880s, Paul Ehrlich observed that intravenous administration of certain dyes (e.g. trypan blue) stained all organs except the brain and the spinal cord. He concluded that the dyes had a lower affinity for binding to the nervous system as compared to other tissues. In 1913, Edwin Goldman, an associate of Ehrlich, demonstrated the very same dyes, when directly injected into the cerebrospinal fluid (CSF), readily stained nervous tissue but not other tissues. The term “blood-brain barrier” was coined, however, by Lewandowsky in 1898, after he and his colleagues had performed experiments to demonstrate that neurotoxic agents affected brain function only when directly injected into the brain but not when injected into the vascular system. It took an additional 70 years until Reese and colleagues localized the barrier to the capillary endothelial cells within the brain by electron-microscopic studies.[4]


So what happens if the blood–brain barrier is damaged or somehow compromised?
One common way this occurs is through bacterial infection, as in meningococcal disease. Meningococcal bacteria can bind to the endothelial wall, causing tight junctions to open slightly. As a result, the blood–brain barrier becomes more porous, allowing bacteria and other toxins to infect the brain tissue, which can lead to inflammation and sometimes death.
It’s also thought the blood–brain barrier’s function can decrease in other conditions. In multiple scleroses, for example, a defective blood–brain barrier allows white blood cells to infiltrate the brain and attack the functions that send messages from one brain cell (neuron) to another. This causes problems with how neurons signal to each other.[5]
Abnormal brain CT
Below are given some examples of anatomical abnormalities and corresponding CT images.
Hydrocephalus
Hydrocephalus is defined as an abnormal collection of CSF within the ventricles of the brain. It is a serious condition, with chronic hydrocephalus causing raised intracranial pressure, and consequently cerebral atrophy.
Based on the underlying cause, there are two clinical classifications:
- Communicating (Non-obstructive) Hydrocephalus – Abnormal collection of CSF in the absence of any flow obstruction in the ventricles. Common causes usually involve the functional impairment of the arachnoid granulations, such as fibrosis of the subarachnoid space following a haemorrhage.
- Non-communicating (Obstructive) Hydrocephalus – Abnormal collection of CSF, with flow obstructed within the ventricular system. The most common site of obstruction is the cerebral aqueduct, connecting the third and fourth ventricles.
There is also a third classification, hydrocephalus ex vacuo – this refers to ventricular expansion, secondary to brain atrophy. This is often seen in patients with neurodegenerative conditions, such as Alzheimer’s disease.[1]
 Hydrocephalus on a CT scan
Hydrocephalus on a CT scan
Extradural and Subdural Haematomas
A haematoma is a collection of blood. As the cranial cavity is effectively a closed box, a haematoma can cause a rapid increase in intra-cranial pressure. Death will result if untreated.
There are two types of haematomas involving the dura mater:
- Extradural – Arterial blood collects between the skull and endosteal layer of the dura. The causative vessel is usually the middle meningeal artery, tearing as a consequence of brain trauma.
- Subdural – Venous blood collects between the dura and the arachnoid mater. It results from damage to cerebral veins as they empty into the dural venous sinuses.[1]

CT scan of a massive extradural haematoma
Cerebellar Dysfunction
Dysfunction of the cerebellum can produce a wide range of symptoms and signs. The aetiology of cerebellar dysfunction is varied, with a number of possible causes. The most common are stroke, physical trauma, tumours and ageing.
The clinical picture is dependent on the functional area of the cerebellum that is affected. Damage to the cerebrocerebellum and spinocerebellum presents with problems in carrying out skilled and planned movements and in motor learning. A wide variety of manifestations are possible:
- ataxia
- dysarthria and scanning speech
- dysmetria (past-pointing)
- hypotonia
- dysdiadochokinesia (difficulty in carrying our rapid, alternating movements)
- inability to learn new movements
- coarse nystagmus
Damage to the vestibulocerebellum can manifest with loss of balance, abnormal gait with a wide stance.[1]
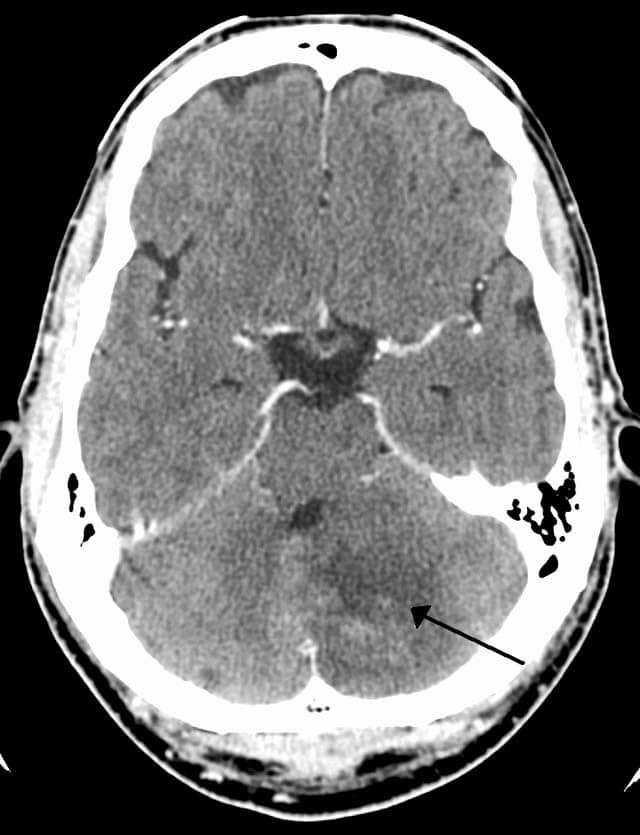
CT scan of a left sided cerebellar stroke.
By James Heilman, MD (Own work) [CCBY-SA 3.0], via Wikimedia Commons
Cerebrovascular Accident
A cerebrovascular accident (also known as a stroke) is defined clinically as “an abrupt loss of focal brain function lasting more than 24 hours due to either spontaneous haemorrhage into brain substance or inadequate blood supply to part of the brain i.e. ischaemia (thrombosis, embolism)“.
Damage to the cerebrum in this matter can give rise to a range of clinical signs. The exact nature of the functional deficit that arises depends on the specific lobe that has been affected:
- Frontal lobe – a diverse range of presentations, often personality and behavioural changes occur and an inability to solve problems develops.
- Parietal lobe – typically presents with attention deficits e.g. contralateral hemispatial neglect syndrome: where the patient does not pay attention to the side of the body opposite to the lesion.
- Temporal lobe – presents with recognition deficits (agnosias) e.g. auditory agnosia: patient cannot recognise basic sounds, prosopagnosia: failure to recognise faces.
- Occipital lobe – visual field defects: contralateral hemianopia or quadrantanopia with macular sparing.
- Global lesions – severe cognitive deficits (dementia), patients cannot answer simple questions such as their name, today’s date, where they are etc.[1]

CT scan of the brain, showing an infarct in the area of the middle cerebral artery.
By INFARCT.jpg: Lucien Monfils derivative work: Suraj (INFARCT.jpg) [CC BY-SA 3.0], via Wikimedia Common
Bibliography
0) Purves D. Et Al. 2004. Neuroscience 3d Edition
1) http://teachmeanatomy.info/
2) http://antranik.org/protection-for-the-brain-meninges-csf-blood-brain-barrier/
3) https://www.learningneurology.com/approach-to-mri-brain/
4) http://neuroscience.uth.tmc.edu/s4/chapter11.html
Kommentar
Unbekannter Benutzer (ga39tec) sagt:
17. Mai 2017You explained the different types and parts of brain regions, but did not mention the hindbrain. Maybe the main regions (forebrain, midbrain, hindbrain) could be explained initially.
In the introductory text, there is is part you probably forgot to take out: „(as pictured on the cover of this book, for example).“
All in all, I think you give a good overview of the forebrain. The hippocampus is explained in both „Basic parts of the brain“ and „The lobes“.
It is a good idea to contain the meninges, the CSF system and the blood-brain-barrier together in „Protection for the Brain“.
You included the history of the blood-brain-barrier, but the historic background is not included in the other anatomy sections.
It is a good idea to give an overview of the abnormites of the brain. I think you picked them randomly, but for randomly picked abnormities they are quite detailed. Maybe this could be a little more structured or more connected to the anatomy part (e.g. for blood-brain-barrier, there is this abnormity, for meninges, there is this abnormity, etc.).
Everything summed up, you created a nice overview of the brain anatomy!