The introduction of robotics in the area of brain surgeries began in 1980, when Kwoh et al [1] performed a robotic brain biopsy. However, it is difficult to properly integrate in the operation room, since numerous ethical questions arise: How much control should the robot have? If something goes wrong, who has ultimate responsibility? Moreover, people still show lots of reticence when it comes to giving this kind of power to a machine, both patients and surgeons. Therefore, current use of robotics in brain tumour surgeries is aimed at improving precision or performing telesurgical operations, and does not offer the robot ultimate control.
Nevertheless, Robots provide unrepeatable advantages. They are extremely stable, provide good accuracy and repeatability in motion, do not get tired and can hold still very precisely for a large period of time. These systems can help eliminate the problem of brain shift by combining imaging and surgery, and can reduce patient trauma by facilitating surgeries through smaller incisions. However, they are "as smart as they are programmed". They lack decision making skills, have limited dexterity, and they are large and expensive. Moreover, the issue of sterility also needs to be taken into account.[2]
From the technical point of view, we can classify surgical robots as passive (which just hold an item) or active (that carry out certain actions). However, most often robots are classified from the point of view of the human-machine interaction, in the following categories: supervisory, telesurgical and shared-control systems. [2]
Supervisory Systems
These systems have the following workflow: the surgeon pre-programs the robot offline, and then the latter carries out the operation, under the supervision of the surgeon.[3]

Image source: [2]
Some of the robots used that fall into this category are:
- Automated Positioning Systems , as well as Radiosurgery systems such as CyberKnife and Gammaknife, discussed previously
- Neuromate[4] (first developed in 1987) is a robot used most usually in stereotactic interventions. The system can be used for biopsy planning, and it provides position feedback from its navigation system (not measured, but calculated), and can carry out ultrasound and CT registration.[5]
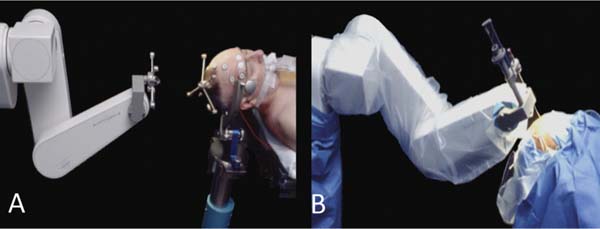
Image source:[6]
- Another system was SurgiScope, that was mounted on the ceiling and could be controlled manually or with a touch-screen controller. Although it is no longer produced and sold, 20 such systems are still in use.[7] The system is also very suitable for navigation without a stereotactic frame, having outstanding neuronavigation functionalities, and can operate in microsurgery or biopsy mode. The system was modular and efficient, but time-consuming and voluminous.[8]
 Image source:[9]
Image source:[9]
- PathFinder is a system with a robotic arm that navigates based on tracking fiducial markers attached to the patient's skull. Registration is don based on CT(for localization) and MRI(for tumour segmentation) datasets. By attaching markers to the robot and using a camera system, Pathfinder could be repositioned in the OR room and it would recalculate the desire path, without the need of a new configuration.[8]
- MKM could work in supervisory or teleguided mode. The system served as a frameless stereotactic navigation system for microscopic image guided surgeries with automatic tool guidance. [8]
Telesurgical Systems

Image source:[2]
These systems are meant to improve the surgeons' dexterity, by filtering and scaling the executed motions, with possible applications for cases when an expert from another location is needed to carry out the procedure.
- The most well-known system of this kind is the Da Vinci system, which is used mainly for gynecologic and general surgeries.
- Another experimental telerobotic system is NeuRobot [10]. The system had to be initially manually positioned, and possibly repositioned during surgery, but it improves precision and force-control. It also needs a stereotactic frame for position registering.[8]
- Neuroarm is a surgical robot designed specifically for neurosurgery introduced in 2008, and it is MR-compatible.[11] The system has 2 arms, 2 cameras and a workstation, and it provides haptic feedback. However, there have been attempts to relate this feedback with tissue properties, but they were unsuccessful[12]. The cost of such a system is around 30 Million USD, and it is not yet commercially available, having been used only ~70 times.
Shared Control Systems

Image source:[2]
- One such system is SteadyHands, developed by Josh Hopkins Institute. The aim of this system is to remove the tremor of the surgeon's hands.
- Another tested system was Evolution 1 developed by Universal Robot Systems, Schwerin Germany. The system was used to guide endoscopic interventions, and it provided positioning precision of 20 um [8]. However, it did not prove to be efficient enough to be consistently introduced to the OR. It has to be repositions 5 cm above the drilling point, and it is very bulky . [2]
Other Experimental Systems
MARS(MiniAture Robotic System)
This robot is meant to insert a needle or a catheter into the brain, and is mounted directly on the patient's skull. It has a 3D surface scanner and performs registration with pre-operative CT or MRI data. Its software was capable of : preoperative planning, surface processing, registration and execution.[8] However, experimental registration results made the robot unable to perform with the precision required for keyhole surgeries.[13] The system has , since 2006, been turned into SpineAssist and has been FDA approved for spine surgery.[14]
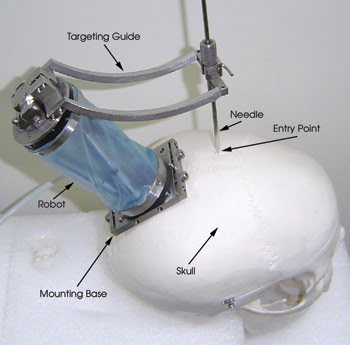
Image source:[15]
ROBOCAST
Robocast is a EU-funded project aimed to develop an intelligent robot that will plan and execute a surgery. Part of this system is the perviously-mentioned PathFinder The robot has too parts(and functionalities): assistance in holding instruments and smooth and precise insertion (which will make up the robot's mechatronic part) , and an intelligence part, that should carry out the trajectory planning (that has to be approved by the surgeon). For the intelligence part, the scientists working on the project have developed a risk atlas, which would help the robot evaluate the safest trajectory to a given point. The robot was planned to be able to carry out not only linear, but also curved trajectories.[16] However, the project website has ended, and the product was not released.
Image source: [16]
ACTIVE (Active Constraints Technologies for Ill-defined or Volatile Environments)
Another EU-funded project, ACTIVE is a robotic platform for neurosurgery that can operate alone or in cooperation with the surgeon. It has two robotic arms, that can be controlled with tele-manipulation or locally ("hands-on"). Its intelligence will limit movements to protect damage to certain areas. Locations and tool monitoring will be done by environmental cameras and machine learning techniques. [17] The system uses 2 7DoF Kuka robots equipped with sensors. The system has a human-authorised safe stopping possibility. Before use, the system has to 'learn' the profile of the surgeon, in order to evaluate the degree of tremor. Flexible probes are being tested for this system.[18]

Image source:[17]
Bibliography:
1)Karas and Baig (2008). "Robotic Neurosurgery, Medical Robotics, Vanja Bozovic " (Ed.), InTech, DOI: 10.5772/5247. Available from: https://www.intechopen.com/books/medical_robotics/robotic_neurosurgery
2)Nathoo N, Cavusoglu MC, Vogelbaum MA et al (2005) "In touch with robotics: neurosurgery for the future", accessed from: https://www.ncbi.nlm.nih.gov/pubmed/15730567 on 15 June 2017
3) "Essentials of Robotic Surgery", edited by Matthew Kroh, Sricharan Chalikonda, accessed from : https://books.google.de/books?id=BGwaBQAAQBAJ&pg=PA2&lpg=PA2&dq=Nathoo+robot+classification&source=bl&ots=_e7hk19c2b&sig=bpwSC2POTGEXzIPKjBj4WnOAzJc&hl=en&sa=X&ved=0ahUKEwjl0o-3o7_UAhWCI1AKHUcZBa0Q6AEIKzAB#v=onepage&q=Nathoo%20robot%20classification&f=false on 15 June 2017
4)http://www.renishaw.com/en/neuromate-stereotactic-robot–10712
5) "Robotic applications in stereotactic procedures are synonymous with speed, safety and efficiency provided a rigorous methodology is followed", Renishaw Case story H-3000-1296-02
6)https://radiologykey.com/neurosurgical-robots-a-review , image courtesy of Qing Hang Li, MD PhD, Wayne State University, Detroit, MI.
7)http://www.surgimedia.com/company/
8)C. Faria, Carlos, et al. "Review of robotic technology for stereotactic neurosurgery.", accessed from: https://repositorium.sdum.uminho.pt/bitstream/1822/39484/1/Faria%20IEEE%20Reviews%20on%20Biomedical%20Engineering%202015_reference.pdf on 15 June 2017
9)http://menzelphoto.photoshelter.com/image/I0000vxqLQyUIKQQ
10)K. Hongo," Telecontrolled micromanipulator system (NeuRobot) for minimally invasive neurosurgery" ,accessed from:
https://www.ncbi.nlm.nih.gov/pubmed/17009702 on 15 June 2017
12)Y. Maddahi, "Treatment of Glioma Using neuroArm Surgical System", accessed from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4895046/ on 15 June 2017
13)L. Joskowicz,Image-guided system with miniature robot for precise positioning and targeting in keyhole neurosurgery, accessed from: https://www.ncbi.nlm.nih.gov/pubmed/17038306 on 15 June 2017
15)https://www.photonics.com/Article.aspx?AID=38428
16)http://www.robocast.eu/index.html
17)http://www.active-fp7.eu/index.html
18) E. de Momi," ROBOCAST and ACTIVE: Advanced Robotic Systems for Neurosurgery" , accessed from: http://emma.polimi.it/emma/events/vdp/attachments/paper_07_04_demomi.pdf
Kommentar
Unbekannter Benutzer (ga38gis) sagt:
17. Juni 2017Good work! It's well structured and nice to read. I like the visualization of the robotic systems you found.
Only some minor remarks: Your "Technical 2" - page is empty, would be nice to have a little overview or at least the links to the subpages. Also the layout of your "Home" is inconsistent (part3&4 bold, part 1&2 not; but I know you still have some days for the details ), and (tiny detail ;)) as the wiki can do greek letters it would be nice, if you write μm instead of um.
), and (tiny detail ;)) as the wiki can do greek letters it would be nice, if you write μm instead of um.