Definition "Robot": A robot is a reprogrammable, computer-controlled mechanical device equipped with sensors and actuators. [1]
Definition "Surgical Robot": A surgical robot is a powered, computer controlled manipulator with artificial sensing that can be reprogrammed to move and position tools to carry out a range of surgical tasks. [2]
In the steadily growing field of information technology, robots play a more and more important role. Many years ago, assembly line workers in industry were replaced by robots and even in daily life, technology, for example in the form of a cleaning robot, simplifies many work steps. In medicine we still mainly rely on “good old manual work”, but robots can simplify many medical procedures. Neurosurgeries taking several hours get simplified fundamentally, as robots never get tired, nor lose focus. Furthermore human hands will never reach the precision and accuracy of robots. However, the integration into the surgical routine is difficult as the safety regulations are strict and there is still deep distrust in robots.
The table below summarizes advantages and disadvantages of surgeons and robots. When using the advantages of both and balancing between the skills of each, the most useful techniques can be found. [1]
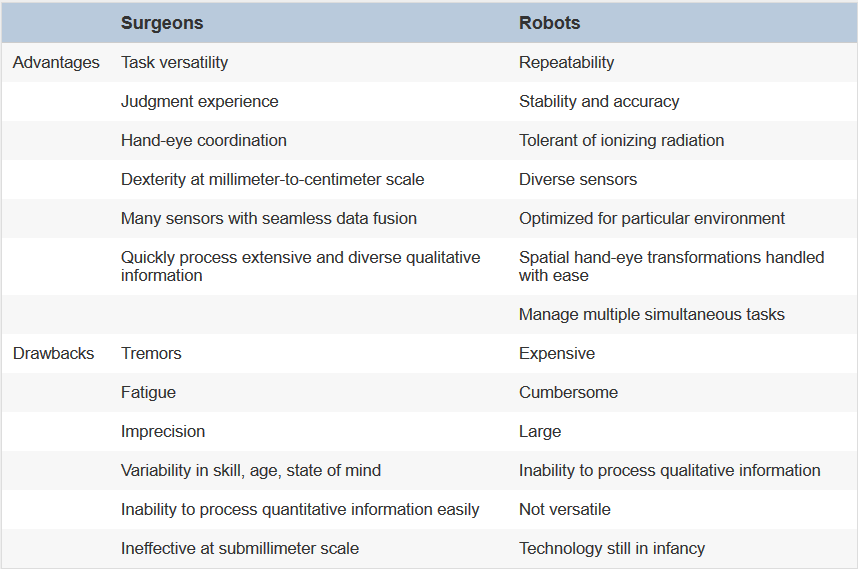
table: Advantages and drawbacks of surgeons and robots.
The First and the Latest Inventions
The very beginning...
The first usage of a robot in neurosurgery was in 1985, when Kwoh used a standard industrial robot (Puma 560) to fixate the patient's head for a biopsy. The role of the robot was the same as of a traditional stereotactic frame, while the surgeon inserted the drills manually. Shortly after this, the company that marketed 'Puma 560' was sold and the new owner refused to allow the robot for surgical purpose. It was considered to be unsafe, as industrial robots are usually used behind a barrier, away from humans. This position has continued with the present owners, though Kwoh's work had indicated that the robot could position itself automatically and very accurately. [2]
Despite the first application of a robot-assisted procedure being in neurosurgery, robotic systems are not as common as in other areas of medicine (urology, cardiology and gastroenterology). This is because of the complex anatomy and the incredibly sensitive tissue found in the brain. [3]
The table below shows some promising systems in neurosurgical robotics, including brain and spine applications that are in use and in development. The systems are further described below.

table: Robotic surgical devices with FDA-approved and experimental neurosurgical applications. [4]
Most recent research: Robotic Skull Base Drill
A recent paper published in May 2017 in the journal "Neurosurgical Focus" describes a computer-aided skull drill that can perform complicated cranial surgeries considerably faster than standard procedures. A surgery time of over 2 hours is done in less than 3 minutes (up to 50 times faster). It was developed by researchers from the University of Utah and it took eight years to get from the idea to the actual appearance in the OR and the commercialization is still going to take some more time. [5]
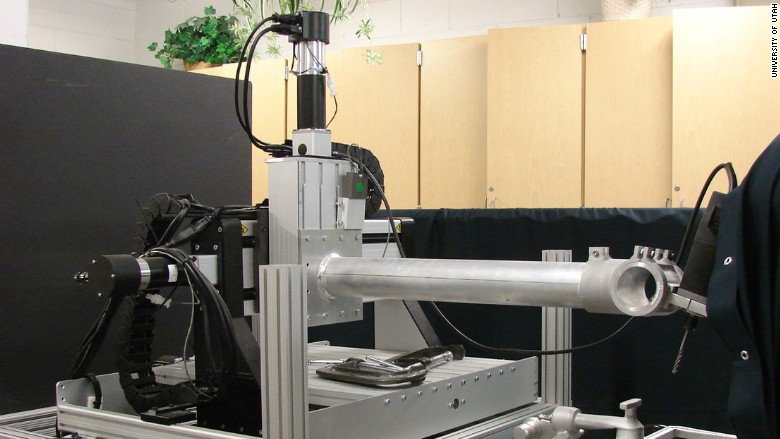
figure: Robotic skull base drill. [6]
The computer-aided design/computer-aided manufacturing (CAD-CAM) device uses an image-guided system to define a cutting tool path in bone that is shared with a surgical machining system for drilling bone. First, 3D CT or MR images are obtained and the precise location of sensitive structures like nerves and major veins is determined. The processor then defines an optimized cutting tool path, which is sent to a surgical machining system that can drill the desired portion of bone (figure below shows method). This tool can be used for precise bone removal in cranial and spine neurosurgeries, especially in the area where a lot of the nerves and the arteries from the brain traverse and go to the face and the arteries come in from the neck. This is necessary if tumors or aneurysms occur at the base of the skull (a particularly difficult procedure that can be handled with the device: acoustic tumor/hearing nerve tumor). [5] [7]
 figure: Schematic of a method for using the automated drill system for surgery (NC = numeric control). [5]
figure: Schematic of a method for using the automated drill system for surgery (NC = numeric control). [5]
The biggest advantage is the massive reduction of surgical time, paired with decreased blood loss and infection risk, as the time the wound is open is reduced. Faster surgeries also mean lower surgical costs (running costs OR, surgeon and nurses salaries, etc.). The device is expected to cost 100,000 $ or less, so in the long-term it is very cost effective. Additionally the time the patient is under anesthesia is much shorter.
In spite of the operating swiftness, the device is very accurate and also the potential for human error is reduced. It is portable, so it can be moved between ORs.
Safety barriers along the cutting path within 1-2 mm of sensitive areas, such as areas of vital functions and major veins, can be programmed. During the procedure a surgeon would stand by and can turn off the device at any time. Additionally the robotic drill automatically shuts off, if it detects it is too close to a facial nerve or other restricted areas.
The tool can also serve as a training tool, it could be used for simpler approaches and to drill out specific bones elsewhere in the body. [5]
Classification
There are some different approaches for classifiing surgical robots, in general it can be based on technology, application, human-machine interaction or role. A technology-based classification might be based on the amount of autonomy, whereas an application-based one might have such categories as cardiology and urology.
Role-based classification: [1]
Passive role: limited scope, low risk-involvement
Restricted role: responsible for more invasive tasks with higher risk, but still restricted scope
Active role: intimately involved in the procedure, high responsibility, high risk
Another approach is classifiing robots by the amount of human-machine interaction: [4]
1. Supervisory-controlled system:
the robotic intervention is preplanned and programmed, it carries out its programmed movements autonomously, supervised by the surgeon

2. Telesurgical (Master-Slave) system:
robot is manipulated by the surgeon in real-time through remote control, with limited feedback to the operator

3. Shared control system:
surgeon directly controls the movements of the robot as the robot enhances the surgeon’s skills through dexterity enhancement (physiologic tremor reduction etc.)
Below, some examples for supervisory-controlled, telesurgical and shared control robotic systems are described.

Supervisory-Controlled Systems
Automated Positioning System (APS)
The Automated Positioning System (APS) (Elekta, Stockholm, Sweden) is used for radiation therapy. APS positions the patient’s head within a collimator automatically, based on a predetermined stereotactic plan. It is an upgrade to the Leksell Gamma Knife radiosurgical system. The benefits are shorter treatment times, reduced exposure of personnel to radiation and reduced maximum dose for the patient due the possibility to deliver radiation to an increased number of smaller isocenters. [4]
NeuroMate and Minerva
The NeuroMate robotic surgical system (Integrated Surgical Systems, Sacramento, CA, USA) was the first FDA-approved robotic device for neurosurgery. Minerva (University of Lausanne, Lausanne, Switzerland) and NeuroMate both consist of a passive robotic arm, which moves in a pre-programmed direction, defined by integrated neuronavigation systems. They are used for stereotactic biopsy or functional neurosurgical applications.
By placing the robotic arm within a CT scanner to provide real-time image guidance, the Minerva project tried to incorporate brain shift correction, but safety issues forced the discontinuation of this device.
NeuroMate provided accurate localization and targeting capabilities and can be used for microelectrode placement for treatment of Parkinson’s disease. [4]
Cyberknife
Cyberknife (Accuracy, Sunnyvale, CA, USA) is a robotic spinal stereotactic radiosurgical system, based on a predetermined plan for focused beam radiotherapy. This system can adjust its trajectory to correct for patient movement (mainly respiration) by use of feedback mechanisms. The usage has been expanded to intracranial use, considering brain shift. An addition to Cyberknife is the RoboCouch Patient Positioning System (Accuracy), which uses similar technology to reposition the patient during the radiation treatment. [4]
SpineAssist
SpineAssist (MAZOR Surgical Technologies, Caesarea, Israel) is a miniature robot coupled with image-guided navigation systems for conventional spinal surgery and has been tested for pedicle and translaminar facet screw placement. The device includes a passive arm, whose motion is defined by preoperatively planned screw trajectories and supervised by a surgeon. SpineAssist is FDA-approved for spinal instrumentation. [4]
Telesurgical (Master-Slave) Systems
Neurobot
The Neurobot is a telerobotic surgical system with multiple arms. It has been used successfully in complex procedures for simultaneous retraction and dissection. For example, it can be used to resect superficial portions of intraaxial tumors in craniotomies. Dexterity enhancement is one of the advantages. [4]
daVinci
The daVinci system is the most well-known telesurgical system, it's mainly used for urologic, gynecologic and general surgeries and it is FDA-approved for those fields. This device has also been tested for several neurosurgical procedures (cadaveric trials of end-to-end ulnar nerve reanastomosis, lumbar discectomy, intradural spinal dissection, complex intraventricular surgery, ..). It provides tremor reduction, motion scaling capabilities, multiple working arms, 3D vision, and Endowrist technology (Intuitive Surgical, Sunnyvale, CA, USA) that allows the flexibility of a human wrist. [4]
NeuroArm
Neuroarm (i.a. University of Calgary, Canada) is a MRI-compatible image-guided computer-assisted neurosurgical robot (introduced in 2008), with two arms, two cameras and a workstation. Interaction forces between the tool tips and the brain tissue are measured and transmitted as haptic feedback to the surgeon. They tried to relate tissue properties with the feedback, but could not find a relationship between forces exerted to the pathological tissue and its size, type, or location. [9] It is not yet commercialized. [10]
Shared Control Systems
Evolution 1
The Evolution 1 robotic system (Universal Robot Systems, Schwerin, Germany) has been tested for several neurosurgical applications. Despite the successful application of Evolution 1, is was considered to be too cumbersome and time-consuming to justify its use. Also is was tested for endoscopic third ventriculostomy (ETV) and showed precision targeting through image-guidance coupling and dexterity enhancement, which eliminates micro movements of a hand-held scope. Even in providing these advances, it has not been introduced into the OR. [4]
ROSA® robotic surgical assistant
ROSA® provides tools for pre-operative planning, automatic instrument guidance, intraoperative navigation and instrument manipulation. It substitutes a stereotactic frame, offers a planning solution based on its platform, might reduce the OR time depending on the procedure and offers increased accuracy and control over procedures. ROSA® can be used for tumor surgery, Parkinson and Epilepsy treatments and endoscopic procedures. [11] [12]

figure: ROSA® robotic surgical assistant. [12]
Robot Characterization
Depending on the task the robot should perform, it needs to be designed accordingly. The following criteria are important to ensure that the robot fits the desired application: [1]
- Degrees of freedom
- Workspace and resolution
- Mechanism type
- Inertia and stiffness
- Speed, force, and backdrivability
- Dynamic range
- Force control versus position control
- Bandwidth
Robots in Science Fiction
The term "robot" was coined in the 1920s by the Czech playwright Karel Čapek. In his satirical drama Rossum's Universal Robots, machines were created to do banal work, but finally the robots became stronger and smarter than their masters and began to exterminate the population. As a response to the play, people became afraid that robots might replace them on the assembly line. Many probing questions arise, which role should robots play in society.
Since then, several famous works displayed robots as fully autonomous anthropomorphic machines (Isaac Asimov's I, Robot, George Lucas' Star Wars, the Terminator movies, ...). Asimov describes in one of his novels the "Three Rules of Robotics” [13]:
- A robot may not injure a human being, or, through inaction, allow one to come to harm.
- A robot must obey all orders given to it from humans, except where such orders would contradict the First Law.
- A robot must protect its own existence, except when to do so would contradict the First Law or the Second Law.
These rules remain a reasonable ethical framework for the development of robots as applied to surgical care. [1]

figure: Karel Čapek's robot in Rossum's Universal Robots. [14]
Outlook - Can Robots Replace Physicians?
Robots play a more and more important role. Many years ago, assembly line workers in industry were replaced by robots and even in daily life, technology, for example in the form of a cleaning robot, simplifies many work steps. A computer in every household has been obligatory for many years now and even more impressively, people are always online, no matter where they are. But in medicine, we still mainly rely on “good old manual work”. So, how can robots or artificial intelligence simplify medical procedures? Or can robots even replace physicians?
In psychotherapy robots are out of the question so far, but in the future it's not inconceivable. There's some evidence that the usage of robots shows success in particular psychological diseases, for example in the therapy of children with autism. Socially assistive robots can teach children with autism valuable social skills like taking turns [15]. On the other hand. especially the progression of psychological diseases is unpredictable and hence unknown terrain for robots. Thus in this field, a physician is still needed, but robots can act as valuable assistants.
A point for the physicians is, who is going to “feed” the robots with new information? Since science hasn't reached the stage yet where artificial intelligence enhances itself (differentiate: self-learning, but not self-enhancing), there is still need for physicians developing new treatment methods. Still unknown diseases and diseases assumed to be incurable are appearing. Since robots are distinct in their behavior, software must be updated regularly with information only human intellect can provide.
The financial aspect also plays an important role. After research and development, only low maintenance costs have to be expected for a robot, whereas a doctor draws his daily salary. Previous work showed a cost reduction of approximately 60% per patient outcome in the field of diagnostics, from treatment-as-usual to artificial intelligence. [16] So in the long term robots might provide a cost-efficient alternative.
The topic “robots“ also includes computer-aided diagnostics. Robots could use worldwide consistent terminology and specific thresholds, for choosing the appropriate treatment. This would immensely promote the global exchange of information. A global disease-database could be created. With every patient, the database is getting bigger and thus the probability to quickly make the right diagnosis is increased. With several hundred documented cases of similar diseases a new treatment can be created. Even for rarer diseases the chances are good to find someone with exactly the same symptoms and so a therapy can be started, which possibly already was successful in the corresponding case. But a computer has neither intellect nor intuition and so it can't react individually to everyone. Sometimes a decision has to be made, before a definite diagnosis is certain. Even more, what happens if something isn't working properly? A misdiagnosis possibly damages more than it helps. And as the computer-aided diagnosis is designed to be trusted, no one questions or controls the decision. The consequences are hard to analyze. To sum up, computer-aided diagnosis definitely has to be taken into account, but as single medical opinion, it must be treated with some caution.
In the field of surgery, robots can be very useful. Operations of several hours get simplified fundamentally, as robots never get tired, nor do they ever lose focus. Human hands will never reach the precision and accuracy of robots. Moreover every single detail is captured, more than what is visible to the naked eye. Previously acquired MRI, PET or other images can be included and simultaneously applied to the robot. So the direct visual information can be superposed and adjusted using those pictures. The realization isn't that easy because every patient has a slightly different anatomy (or even very different anatomy in the case of situs inversus). But with further research it is conceivable that robots will do surgeries autonomously one day.
An advantage of physicians is that the psychological, emotional component between doctor and patient is lacking when talking to a robot. Psychological care must not be underestimated and can't easily be replaced by artificial intelligence. Interaction with the doctor is a part of the treatment, a positive attitude and especially laughing is evidentially beneficial to the healing [17]. As of now, robots can't substitute the emotional component of the cure, but who knows what the future will bring.
Medical treatment is a sensitive topic patients will not easily lay in the hands of robots. A problem for the design of humanoid robots is the so called “uncanny valley”, first described by Masahiro Mori. “Uncanny valley” is a hypothesis which states that affinity and human likeness of robots are first increasing steadily with each other. When a certain point is reached, the familiarity quickly switches completely into revulsion. If robots become almost indistinguishable from humans, familiarity increases again (figure below). [18] So, to win the patient's confidence, a cautious approach is necessary, when designing a medical robot.

figure: Uncanny Valley. Proposed relation between human likeness of robots/puppets and the observer's affinity for it (note: Bunraku is a traditional Japanese form of musical puppet theater) [19]
Another aspect in favor of robots is that robots can also serve as monitoring devices. They could go along with the patient all day long and prohibit incorrect drug use, for example by reminding the patient at the right time. So they can even give a feeling of security. An example for smartphone-based monitoring is a project of the TUM to develop a cognitive medical system. While measuring for example blood pressure, weight and activity, this offers a mobile diagnostics and therapy platform [20]. Moreover robots can intervene if a doctor prescribes the wrong medication and can simultaneously check the drug interaction between the different administered medications in the database.
To sum up, robots as monitoring devices are a great opportunity.
At the moment robots alone seem not to be the solution, but humans also can achieve little without technology. In the future it might be possible that robots replace physicians in certain medical areas, but it's rather improbable that the whole of medical personnel will be redundant some day.
Finally it can be stated, that until now it's not a human versus robot decision but rather the question how human-robot collaboration can be improved and improved the most. Computer-aided diagnostics can be seen as rather a second medical opinion or even the first one, but up to now physicians have the final say.
Bibliography
1) Camarillo D.B. et al. (2004) Robotic technology in surgery: past, present, and future, The American Journal of Surgery, http://www.americanjournalofsurgery.com/article/S0002-9610(04)00375-7/fulltex
2) Davies B. (2000) A review of robotics in surgery, Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine, http://journals.sagepub.com/doi/abs/10.1243/0954411001535309
3) Campbell S. (April 2017) The impact of robotic-assisted surgery and engineering on neurosurgery, Engeneers Journal, http://www.engineersjournal.ie/2017/04/24/impact-robotic-assisted-surgery-engineering-neurosurgery/ (access 17/06/17)
4) Karas C.S. et al. (2007) Neurosurgical robotics: a review of brain and spine applications, Springer London, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4247436/
5) Coulwell W.T. (May 2017) Computer-aided design/computer-aided manufacturing skull base drill, Neurosurgical Focus, JNS, http://thejns.org/doi/full/10.3171/2017.2.FOCUS16561
6) CNN tech, http://i2.cdn.turner.com/money/dam/assets/170430212651-automated-robot-drill-780x439.jpg (access 17/06/17)
7) Interview with Coulwell W.T. (June 2017) Health Care Insider: From Concept to Reality-Robotic Brain Surgeon Drill, University of Utah Health, https://healthcare.utah.edu/the-scope/shows.php?shows=0_8xvw01cf (access 17/06/17)
8) Ways of using robotic neurosurgery, http://callisto.ggsrv.com/imgsrv/FastFetch/UBER1/ZI-1ZOX-2013-ANN00-IDSI-153-1 (access 18/06/17)
9) Maddahi Y. et al. (2016) Treatment of Glioma Using neuroArm Surgical System, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4895046/ (access 18/06/17)
10) neuroArm, http://www.neuroarm.org/ (access 18/06/17)
11) ROSA® Brain, Medtech, http://www.medtech.fr/en/rosa-brain (access 18/06/17)
12) Medtech (2016) ROSA® Brain Brochure, accessed via http://www.medtech.fr/en/rosa-brain (access 18/06/17)
13) Asimov I. (1982) The Complete Robot, Doubleday, Garden City, NY
14) RUR, http://robotics.cs.tamu.edu/dshell/images/rur.jpg (access 16/06/17)
15) Weir K (2015) Robo therapy, american psychological association, http://www.apa.org/monitor/2015/06/robo-therapy.aspx (access 17/06/17)
16) Bennett et al. (2013) Artificial Intelligence Framework for Simulating Clinical decision-making: A Markov Decision Process Approach, Artificial Intelligence in Medicine
17) Laughter therapy, Cancer treatment centers of america, http://www.cancercenter.com/treatments/laughter-therapy/ (access 17/06/17)
18) Mori M. (1970) The Uncanny Valley, Energy
19) Spectrum IEEE, http://spectrum.ieee.org/image/MjA3NjMzOQ.png (access 17/06/17)
20) New therapeutic options with COMES (2012) TUM, Fakultät für EI, Heinz-Nixdorf-Lehrstuhl für Medizinische Elektronik, https://www.lme.ei.tum.de/index.php?id=141&L=1 (access 17/06/17)
Kommentar
Unbekannter Benutzer (ga94leq) sagt:
21. Juni 2017Sorry for being a bit late but here is my feedback: I like the organisation of the page and the flow of the information. I really liked your outlook regarding "Can robots replace physicians", i found it really interesting. Nicely done!